A six-year national effort found that more than 70% of patients with higher-risk findings received one-on-one genetic counseling, but disparities in access remain a concern.
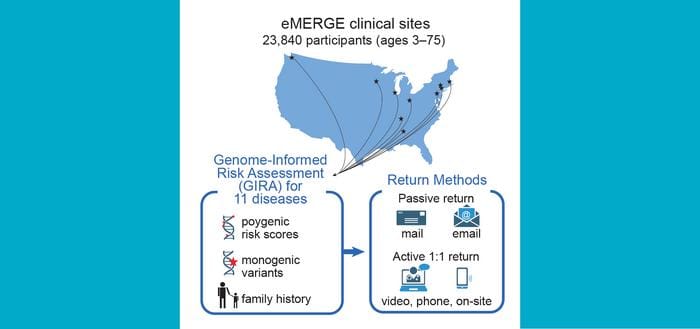
A new study published in the American Journal of Human Genetics offers a look at how genetic risk information can be returned to patients at scale—and where health systems still fall short. The research, conducted through the eMERGE network, a multi-site genomic medicine initiative, tracked the return of genome-informed risk assessments to nearly 24,000 adults and children across 10 participating medical centers.
The findings arrive as clinical laboratories and health systems face growing pressure to translate advances in polygenic risk scoring into actionable patient care—while navigating complex ethical, logistical, and equity challenges.
What the Study Examined
Researchers tested nearly 24,000 people, ages 3 to 75, for their genetic risk of developing any of 11 common health conditions. The conditions included asthma (pediatric only), type 1 diabetes (pediatric only), obesity, type 2 diabetes, atrial fibrillation (adult only), chronic kidney disease (adult only), heart disease (adult only), high blood cholesterol (adult only), colorectal disease (adult only), prostate cancer (adult male only), and breast cancer (adult female only).
Results were shared using a tiered communication approach. Patients with lower-risk findings received results via secure electronic messages or by mail. For nearly 5,000 patients with higher-risk findings, however, the research team attempted to deliver results through direct, one-on-one conversations—conducted by phone, video call, or in person.
More Than 70% Reached, but Gaps Remain
The team successfully completed one-on-one conversations with approximately 79% of adult participants and 68% of pediatric participants who had higher-risk results. First author Lucinda Lawson, PhD, of Cincinnati Children’s Hospital Medical Center, worked with researchers across all 10 eMERGE sites to document both the successes and the barriers.
“We were able to complete one-on-one conversations with about 79% of adults and 68% of children,” says Leah Kottyan, PhD, co-lead of the Cincinnati eMERGE team, in a release. “Our biggest challenge was also the simplest: sometimes the team simply could not reach participants.”
When patients with higher-risk findings could not be reached directly, their results were still uploaded to their electronic medical records, along with contact information for the research group so clinicians and patients could follow up.
Disparities in Who Got the Call
The study also examined what factors predicted whether a patient successfully completed a one-on-one conversation. Researchers found that people with markers of greater socioeconomic stability—such as higher educational attainment or homeownership—were more likely to complete a session. Insurance status was also a differentiating factor.
These findings raise concerns for laboratorians and genomic medicine specialists thinking about equitable implementation of genetic testing in clinical practice. If the patients most likely to benefit from early intervention are also the least likely to receive their results through a direct conversation, the promise of precision medicine may not be distributed equally.
“These findings show that returning genetic risk information at this scale is possible,” says Kottyan in a release. “However, health systems will need better, more flexible ways to contact and support patients so that everyone can benefit equally—especially when the results are higher-risk and may lead to earlier screening, prevention steps, or follow-up care.”
A Blueprint for Clinical Labs and Health Systems
The eMERGE study offers a framework for how clinical laboratories and health systems might structure genetic result disclosure workflows going forward. The tiered communication model—with passive delivery for lower-risk findings and active outreach for higher-risk ones—provides a scalable starting point, though the researchers acknowledge it requires significant coordination and resources.
Ongoing analyses will examine how clinician and patient behaviors differ between groups that did and did not receive a one-on-one conversation, which could yield further guidance on best practices for return-of-results protocols in both research and clinical settings.
The study was supported by the National Human Genome Research Institute (National Human Genomic Research Institute). Co-authors spanned more than 20 institutions, including Boston Children’s Hospital, the Broad Institute, Brigham and Women’s Hospital, Children’s Hospital of Philadelphia, Columbia University, Harvard University, the Icahn School of Medicine at Mount Sinai, Invitae (now part of Labcorp), Massachusetts General Hospital, Mayo Clinic, the Medical College of Wisconsin, Northwestern University, Tulane University, the University of Alabama at Birmingham, the University of Washington, Vanderbilt University, and the Washington State Department of Health, among others.
Photo caption: Illustration shows pathways the participating eMERGE network members followed for sharing results from genetic risk tests.
Photo credit: eMERGE Network
Related Articles:
DPYD Testing Gaps Leave Colorectal Cancer Patients at Risk for Severe Drug Toxicity
Study Finds Multi-Omic Breast Cancer Test Predicts Radiation Therapy Benefit




{kind=link}