
The future of precision medicine depends on IT-enabled pharmacogenomic testing
By Don Rule
As healthcare providers seek to understand how an individual’s unique genomic makeup predicts their response to prescribed drugs, the use of pharmacogenomic testing continues to grow. New technologies and the availability of cost-effective methods for the interpretation of genetic test results are advancing the use of pharmacogenomic testing, so that clinicians can prescribe the right medication for precise treatment with less trial and error.

Don Rule, Translational Software.
When integrated with patient data from electronic health record (EHR), e-prescribing, and laboratory information management systems, a pharmacogenomic profile can be used to help ensure the best treatment and outcomes by delivering testing prompts, genomic-based alerts, and actionable decision support at the point of care.
To optimize the implementation and potential benefits of a pharmacogenomic testing program, significant consideration should be given to choosing the right pharmacogenomic test menu, educating healthcare providers and patients, and seamlessly integrating pharmacogenomic data and clinical decision support (CDS) systems into existing clinical processes and systems.
Choosing a Target Pharmacogenomic Test Menu
Since numerous actionable pharmacogenetic variants are known to exist across a number of genes—and more are being uncovered or are under investigation—an important decision that must be made early on is which gene-drug pairs and genetic mutations a laboratory’s pharmacogenomic testing program will target. To ensure the greatest utility and return on investment, it is best to focus on gene-drug pairs that are relevant to current clinical initiatives, with a high clinical correlation to the organization’s patient mix, or that target key patient populations.
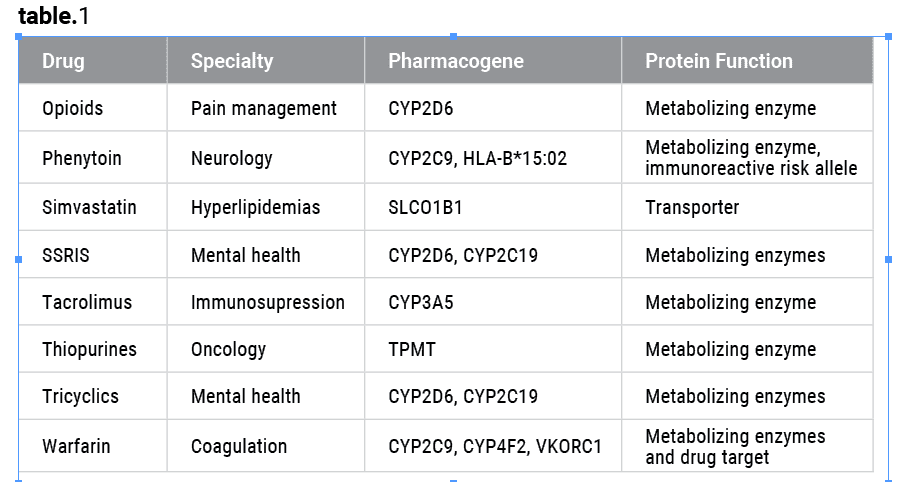
Table 1. Example of gene-based guidelines issued by the Clinical Pharmacogenetics Implementation Consortium. Click to expand.
The primary consideration is how the laboratory’s test results will be used to influence clinical decisionmaking and improve outcomes. In the case of FDA-approved drugs, the instructions for use may require testing with a companion diagnostic, or recommend the use of a complementary pharmacogenomic test.1 In addition, laboratories should consider using clinically actionable genetic variants and drugs with evidence-based practice guidelines already established by professional societies or pharmacogenomics consortia such as the Clinical Pharmacogenetics Implementation Consortium (CPIC).2 These guidelines are designed to help clinicians understand how available genetic test results should be used to optimize drug therapy (see Table 1). Gene-drug pairs that are the subjects of a clinical practice guideline are based on several criteria and take into consideration:
- FDA labeling that requires or recommends pharmacogenomic testing prior to therapy initiation.
- Evidence of reimbursement for the test from public and private third-party payors.
- Clinical trials demonstrating drug effects linked to functional pharmacogenomic loci.
- Narrow therapeutic index drugs (ie, those with a low ratio between toxic dose and therapeutic dose).
- Availability of safer and therapeutically equivalent alternatives for drugs associated with a pharmacogenomic concern.
- Support of testing from professional organizations (eg, American Heart Association, American Society for Clinical Pharmacology and Therapeutics, American Society of Clinical Oncology).
Educating Physicians and Patients
A key challenge for implementing a pharmacogenomic testing program is how to provide adequate education to physicians regarding what tests may reveal and what they will not, how to interpret the results, and how to integrate findings into clinical care.
Beyond the usual run of in-service training and continuing education activities, organizations can provide physician education in a number of ways. Leading healthcare organizations that have implemented pharmacogenomic services have found it helpful to create websites that include pathways to information for both physicians and patients. Such sites commonly provide information describing the pharmacogenomic service; which genes are being tested; how the information will be used; key literature, videos, and FAQs; and who to contact for additional information. Preferably, professionals with training in genetics and pharmacology should also be made available, either onsite or through referral mechanisms, to provide additional information and support as needed.
Laboratories can also play a vital role in helping clinicians order and interpret genetic tests by supporting the use of genomic decision support tools within the clinical workflow. Such tools take into account the patient’s current medication list, pharmacogenetic profile, and other factors, in order to guide clinical decisions about which tests and drugs are most appropriate for the patient.
Aside from providing educational materials, laboratories should also give significant consideration to the question of when and how test results should be communicated to patients. Since pharmacogenomic test results provide a benchmark that will remain relevant throughout a patient’s lifetime, the results should be discussed with the patient prior to discharge. The results should be permanently stored in the patient’s EHR, or an ancillary system, where they can be available for future access. A copy of the results may also be provided to the patient and forwarded to the patient’s primary care physician.
The field of pharmacogenomic testing is advancing rapidly, and it is common that new information or recommendations are available that did not exist at the time of initial reporting. When this information relies on genotypes that were already tested, it is straightforward to provide new reports or alerts at the time of a medication therapy management consultation or during reconciliation for a transition of care. Although new variations of genes are still being discovered, most commercial tests today focus on specific actionable variants, so pharmacogenomic tests do not typically report out variants of unknown significance that must be reconciled later.
Implementing an Information Technology Infrastructure
The healthcare industry is making significant strides in the development and use of new information technologies (IT) for processing and managing the genomic information needed for precision medicine initiatives.
Among recent advances in this area are pharmacogenomic-based application programming interfaces (APIs) developed using the fast healthcare interoperability resources (FHIR) specification, a new open-source standard for ensuring interoperability and security while exchanging healthcare information. FIHR-based APIs are enabling health systems, laboratories, and software developers to accelerate the development of pharmacogenomic-enhanced applications via plug-and-play access to existing pharmacogenomic knowledge platforms.3
In the traditional model where laboratories provide reporting, the test results are on paper and are available to the initial recipient or anyone who has received a copy. With pharmacogenomic tests, the initial test report may have been restricted to medications of interest to the ordering physician, but the genomic test data may be relevant to a much wider field of use. Consequently, it is important that the test results remain accessible to query well after the initial report. While some EHRs have the capability to store data for later use, there is little standardization for the format of such data or how they will be retrieved by a CDS system. Until such standardization occurs, one alternative is a third-party repository that makes the data available to application programmers through secure services. How permissions are provided and how authorization is granted are areas of evolving uncertainty.
When implementing such IT systems, labs will need to evaluate a number of important workflow, process, and systems considerations, beginning with the clinical pathway where pharmacogenomic testing will be introduced within the organization’s information system infrastructure, (eg, at the point of a lab order, or at the point of a prescription order). Other considerations to be addressed include how physicians will receive decision-support alerts when a patient’s pharmacogenomic information should be used to inform and personalize care decisions, and where the patient’s pharmacogenomic test results will be permanently stored.
Integrating pharmacogenomics intelligence for clinician access through web-based portals or via EHR systems is an important task, as it fulfills regulatory requirements protecting the privacy and security of health information established by the Clinical Laboratory Improvement Amendments of 1988 (CLIA), and the Health Insurance Portability and Accountability Act of 1996 (HIPAA).4,5
One of the IT backbones of an effective pharmacogenomic testing program is a CDS capability that automatically translates complex pharmacogenomic data into information that is actionable for a clinician. This information, in the form of reports or alerts, provides physicians with the intelligence they need to order pharmacogenomic tests, interpret test results, and choose safer and more-effective medications (see
“Improving Test Interpretation with Visual, Decision-Ready Reports“). A genomics-based CDS that is integrated into existing ordering or prescribing systems can be used to:
- Screen patient populations for individuals who are likely to benefit from a pharmacogenomic test.
- Identify patients who may be candidates for a pharmacogenomic test when a specific medication is being considered.
- Easily and quickly order the appropriate pharmacogenomic test panel.
- Receive alerts about potential gene-drug and drug-drug interactions and adverse events, and access medication and dosage alternatives.
- Access genetic test results to flag potential interactions as the patient’s medication list evolves throughout their lifetime.
The operative word for ensuring the success of such CDS capabilities is ‘actionable.’ Overalerting with confusing or irrelevant information can result in physicians ignoring or overriding alerts that are important for improving care.
Coverage and Reimbursement of Pharmacogenomic Tests
Payor coverage is a key consideration influencing the adoption of pharmacogenomic testing in clinical practice. Despite the potential for pharmacogenomic testing to improve health outcomes and costs by identifying an individual’s response to medications and supporting gene-guided therapies, payors can be cautious in their coverage of genetic tests, and reimbursement practices vary widely (see “Pharmacogenomics in Clinical Practice“).
National payors and health plans use a variety of data sources to help determine their policies and criteria for the coverage of pharmacogenomic testing, typically emphasizing clinical and economic evidence that a genetic test will directly affect treatment or result in better outcomes.6 Payors often consider FDA market authorization as the essential prerequisite for covering a pharmacogenomic test that will influence the prescription of common medications. But they also use well-recognized guidance from professional societies such as CPIC, which produce evidence-based information to help establish the clinical validity and utility of genetic tests.
In spite of the availability of such guidelines and recommendations from regulatory agencies and professional societies, however, payors do not universally or consistently follow such sources when deciding whether to cover genetic testing. Many payors cover genetic testing selectively if the patient meets defined criteria and obtains prior authorization. Some genetic tests are considered experimental or investigational because of the perceived lack of evidence concerning their safety or efficacy.
Reimbursement decisions about genetic testing are also complicated by a lack of outcomes data evaluating the economics of pharmacogenomics. Several government agencies are working toward the development of regulatory standards for genetic testing laboratories and the integration of genetic testing into routine medical care. The Centers for Disease Control and Prevention has an advisory group focused on the CLIA program, with projects under way to validate genetic tests and their integration into clinical practice. In addition, the National Human Genome Research Institute (NHGRI) is a resource for payors in their evaluation of emerging genomic tests for reimbursement, and promotes research into the benefits and cost-effectiveness of genomic testing.7
To help obtain reimbursement of claims for genetic tests in a reliable and consistent manner—and to avoid denied claims—labs need to comply with the specific evidence and reimbursement criteria and related documentation requirements established by payors for the pharmacogenomic tests offered, and submit claims according to established policies.
A genomics-based CDS is an indispensable tool for helping clinicians determine which tests are reasonable and necessary, and producing the patient-specific clinical evidence needed to inform payors that a pharmacogenomic test is clinically indicated. A CDS can help expedite the use of valuable pharmacogenomic data in clinical practice by identifying patients for whom a genetic test is appropriate, quickly interpreting complex test results, and providing actionable therapy recommendations for the patient.
Conclusion
It is anticipated that the use of genomic decision support tools will become the standard of care in support of evidence-based, precision medicine. Such systems will provide a means of substantiating treatment decisions and guiding better cost and health outcomes for patients, providers, and payors alike.
Unquestionably, the initial impact of pharmacogenomic testing is greatest at the point of care, where test results can guide the physician’s decisions toward improved patient outcomes. But the future of precision medicine also requires an information system infrastructure that provides the ability to store, access, and flag pharmacogenomic test results over the lifetime of the patient. Long-term use and analysis of such data will inform the development of better patient care regimens for use by all healthcare providers.
Don Rule is CEO of Translational Software Inc., Bellevue, Wash. For further information, contact CLP chief editor Steve Halasey via [email protected].
References
- List of cleared or approved companion diagnostic devices (in vitro and imaging tools) [online]. Silver Spring, Md: Center for Devices and Radiological Health, FDA, 2017. Available at: www.fda.gov/medicaldevices/productsandmedicalprocedures/invitrodiagnostics/ucm301431.htm. Accessed March 16, 2017.
- Relling MV, Klein TE. CPIC: Clinical Pharmacogenetics Implementation Consortium of the Pharmacogenomics Research Network. Clin Pharmacol Ther. 2011;89(3):464–467; doi: 10.1038/clpt.2010.279.
- Welcome to FHIR [online]. Ann Arbor, Mich: Health Level Seven International, 2016. Available at: www.hl7.org/fhir/index.html. Accessed March17, 2017.
- Clinical Laboratory Improvement Amendments of 1988. 42 USC 263a (PL 100-578). Available at: www.gpo.gov/fdsys/pkg/statute-102/pdf/statute-102-pg2903.pdf. Accessed April 30, 2017.
- Health Insurance Portability and Accountability Act of 1996. 42 USC 300gg, 1181 et seq., and 1320d et seq. (PL 104-191). Available at: www.gpo.gov/fdsys/pkg/plaw-104publ191/pdf/plaw-104publ191.pdf. Accessed April 30, 2017.
- Genetic testing: Pharmacogenetics [online]. Bloomington, Minn: HealthPartners, 2017. Available at: www.healthpartners.com/public/coverage-criteria/genetic_testing_pharmacogenetics.htm#administrative-process. Accessed March 28, 2017.
- Vozikis A, Cooper D, Mitropoulou C, et al. Test pricing and reimbursement in genomic medicine: towards a general strategy. Public Health Genomics. 2016;19(6):352–363; 10.1159/000449152.



{kind=link}