Summary:
A recent study demonstrated that ATR-FTIR spectroscopy can accurately differentiate normal, benign, and malignant breast tissues using specific biomarker ratios, showing high sensitivity and diagnostic potential.
Takeaways:
- High Diagnostic Accuracy: The cytoplasm-nucleus ratio and glycogen markers achieved AUC values up to 1.00, with 100% sensitivity in distinguishing various breast tissue types.
- Effective Tissue Classification: ATR-FTIR spectroscopy successfully distinguished normal from malignant and benign tissues, and also discriminated between benign subtypes like fibroadenoma and fibrocystic changes.
- Clinical Promise with Limitations: While results are promising, especially for biomarker-based classification, further studies with larger cohorts are needed to confirm clinical applicability.
Histopathology is the gold standard in cancer diagnosis. However, attenuated total reflectance (ATR)-Fourier transform infrared (FTIR) spectroscopy has shown diagnostic potential in other settings. A recent study was aimed at investigating the sensitivity and specificity of the ATR-FTIR spectroscopy in evaluating breast lesions.
Formalin-Fixed Paraffin-Embedded Biopsy Blocks Used in Study
The study was conducted on formalin-fixed, paraffin-embedded biopsy blocks received at Ladoke Akintola University of Technology Teaching Hospital between 2022 and 2023. The blocks were categorized into 10 normal (from benign breast tissue), 15 benign, and 31 malignant samples. Tissue sections of 15 µm were obtained during block trimming and floated onto FTIR slides. An additional 4 µm tissue sections were stained with hematoxylin and eosin for tumor diagnosis and to identify suitable areas on the FTIR slide. Spectrometer readings were taken within the range of 4000–600 cm−1, 32 scans, and 16 cm−1 resolution, using the average of 10 preprocessed spectra per slide. Biomarkers were calculated by ratioing peak intensities for A1632/A1543, A1632/A2922, A1632/A1080, A1080/A1543, A1237/A1080, and A1043/A1543, which represent protein, diagnostic marker, cytoplasm-nucleus ratio, carcinogenesis marker, phosphate, and glycogen, respectively. The receiver operating characteristic curve was used to determine sensitivity, specificity, and the area under the curve (AUC).
Malignant vs. Benign Tissue Effectively Distinguished
The AUC analysis showed that cytoplasm-nucleus ratio values of 0.99 and 0.95 effectively distinguished normal from malignant tissue, and benign from malignant tissue, respectively (p < 0.0001). Additionally, protein marker (AUC = 0.73), diagnostic marker (AUC = 0.85), and cytoplasm-nucleus ratio marker (AUC = 0.94) were able to discriminate normal from benign tissue. Overall, the receiver operating characteristic analysis showed 100% sensitivity and specificity ranging from 54% to 87%. Glycogen (AUC = 1.00) exhibited 100% sensitivity in discriminating fibroadenoma from fibrocystic changes.
ATR-FTIR Spectroscopy Demonstrates Remarkable Diagnostic Accuracy
The study examined the efficacy of ATR-FTIR spectroscopy in distinguishing between normal and abnormal breast tissues using specific peak ratios as biomarkers. The research highlights that certain biomarkers, particularly the nucleocytoplasmic marker, demonstrate remarkable diagnostic accuracy, achieving an AUC ranging from 0.9 to 1.0, with a sensitivity of 100% in differentiating normal, benign, and cancerous tissues. Glycogen is identified as the most effective discriminator between fibrocystic changes and fibroadenomas, also showing perfect sensitivity and specificity. However, there is a need for future research with larger sample sizes to validate these findings.
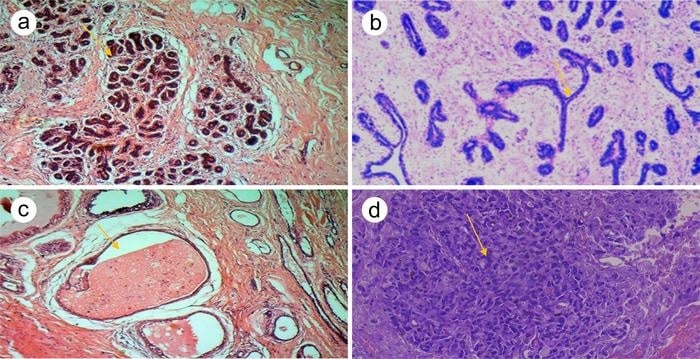
Featured Image: Haematoxylin and Eosin stained photomicrographs of (a) normal breast tissue section with lobules containing dark blue-stained acini nuclei (black arrow), separated by denser collagen fibers, compared with the stroma that separates the lobules ×400. (b) Breast lobules compressed into a slit-like shape (star-black arrow) due to excessive growth of the intervening stroma that separates the lobules (Fibroadenoma) ×400. (c) Cystic breast tissue with two large cysts (black arrow) filled with pink-staining amorphous material, lined by a single layer of epithelial cells ×400. (d) Invasive ductal carcinoma (Not Special Types).
This case was Nottingham grade II. Note the number of tubule formations, high pleomorphism, and mitotic figures in the picture ×400. Image: Samuel T. Adeleke



{kind=link}