
Prompt POC testing is key for improving patient treatment
Interview by Steve Halasey
At this time of year, it should be no surprise to laboratorians that reports from the Centers for Disease Control and Prevention indicate a nationwide increase in the rate of influenza activity. According to the agency’s report for the last full week of 2018, this winter’s flu season is beginning to pick up, with all 10 of the agency’s regions reporting outpatient visits for influenza-like illness at or above their region-specific baselines.
But the predictable arrival of each winter’s flu season still catches many Americans off guard and without the protection they might receive from an annual flu vaccination. And when a winter illness does arise, many people are uncertain about what to do next. One clear recommendation has emerged from this annual cycle: when in doubt, patients should get tested to determine the nature of their illness. Modern flu tests can go a long way to ensure that patients are treated promptly and correctly—but the first step is to use them. To find out more about how influenza diagnostics are helping to improve patient treatment during the current flu season, CLP recently spoke to Troy Hopps, global platform leader for point of care at BD Diagnostic Systems, San Diego.
CLP: In spite of strong encouragement from the provider community, in the United States the rate of vaccination against the flu remains relatively low. Why is that?
Troy Hopps: Historically, only about 40% of adults between the ages of 18 and 65 get a flu shot annually—despite encouragement from the healthcare community and educational efforts to convey the benefits of vaccination.1 There is a general perception among members of the public that the flu vaccine is not very effective at preventing infection, and some patients therefore refrain from getting vaccinated. It is true that the flu vaccine may not prevent disease in all vaccinated individuals. Nevertheless, it is well documented that vaccination reduces the severity of infections and complications associated with influenza.
CLP: Do patients generally understand the difference between bacterial and viral infections, and the different methods required to treat them?
Hopps: While patients may understand the basic difference between bacteria and viruses, we should not expect them to be able to determine the cause of an infection based solely on physical symptoms, which can be very similar for bacterial and viral infections. Ailments such as runny nose, cough, sore throat, and a mild fever are common to both influenza and bacterial infections. Thus, it is imperative that patients get tested as soon as possible—preferably within 48 hours of developing symptoms—as this provides the optimal window for receiving effective treatment, such as antiviral medication in the case of influenza.2–4
CLP: Healthcare providers certainly understand the differences between bacterial and viral infections, so why are so many such infections treated incorrectly—and ineffectively?
Hopps: Because the signs and symptoms of common bacterial and viral respiratory infections are often similar or indistinguishable, early and accurate diagnosis poses an ongoing challenge for healthcare professionals.
Diagnostics—and particularly the use of point-of-care tests—can provide healthcare professionals with the critical information they need to make appropriate treatment decisions for their patients. Specifically, a fast and correct diagnosis will help prevent inappropriate use of antibiotics or antiviral medications, as well as unnecessary ancillary testing. Such diagnostic testing will also support more-effective decisionmaking with regard to hospital admissions and emergency department referrals, which in turn can aid in reducing unnecessary healthcare costs.5,6
CLP: What is the effect of such inappropriate treatments on the rise of antimicrobial resistance?
Hopps: It has been clearly demonstrated that antibiotic use is the primary driver of antimicrobial resistance and leads to adverse events ranging from allergic reactions and diarrhea to Clostridium difficile infections.7 Out of the 262 million outpatient antibiotic prescriptions dispensed in the United States each year, it is estimated that only 70% are appropriate.8,9 And every year, at least 2 million people in the United States get an antibiotic-resistant infection, and at least 23,000 people die.10
CLP: How do diagnostic tests help healthcare providers to ensure that flu patients receive the correct treatment?
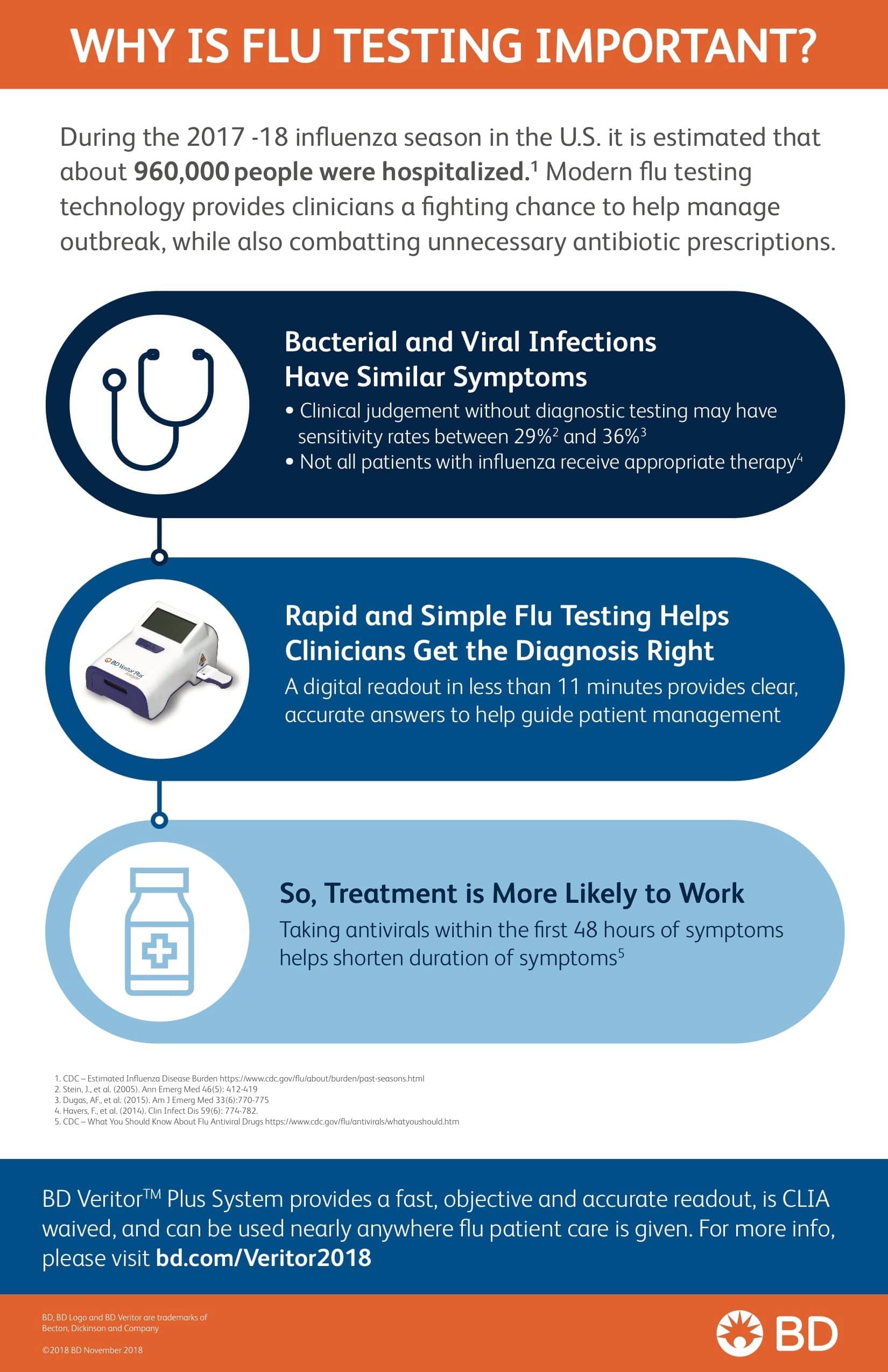
BD infographic explains the benefits of rapid flu testing at the point of care.
Hopps: During the respiratory infection season, which occurs during the winter months, most healthcare providers see a steady flow of patients with flu-like symptoms. Because respiratory infections with different causes often present with similar symptoms, however, it is common that providers struggle to make a correct diagnosis.
Nevertheless, it is essential that providers develop a correct diagnosis, so that they can provide appropriate patient management in a timely manner. Infections such as influenza, respiratory syncytial virus (RSV), and strep pharyngitis each suggest treatment considerations that are distinct from those appropriate for other respiratory infections, so it is helpful for providers to be able to diagnose such infections accurately.
Healthcare practices are best served by diagnosing and identifying treatments during a single consultation, thereby reducing the need for follow-up visits or communications. Point-of-care tests, and especially rapid digital immunoassays (DIAs), can produce results in less than 11 minutes, can streamline the point-of-care diagnostic workflow, and can enable providers to quickly review patient results in order to assist in determining the appropriate treatment during a single consultation.11
CLP: How important is it that current diagnostic systems can provide test results in a matter of minutes?
Hopps: The ability to quickly diagnose influenza in an outpatient setting allows healthcare providers to avoid repeat testing, decrease the burden on hospitals and emergency rooms, and initiate the correct treatment while also advancing antibiotic stewardship. Fast diagnosis also enables healthcare providers, patients, and caregivers to address the possibility of further spread of the disease, sometimes by prescribing prophylactic therapy for vulnerable close contacts of the patient, all within a single consultation.
Both influenza and RSV result in substantial morbidity and mortality every year, particularly among children and high-risk individuals. Given the difficult nature of making a diagnosis based solely on clinical symptoms, it is critical that specific diagnostic tools are utilized to better declare diagnoses and assign treatment protocols.12
CLP: In your experience, where are most patients tested for flu? Do current test methods help to support the optimal sites and timing for such testing?
Hopps: Most patients with acute respiratory tract infections present in ambulatory care settings. The BD Veritor system, which is an example of a rapid digital immunoassay, is commonly used in physician office labs, retail clinics, and emergency departments, and as a rapid screening test in hospital core labs. Such tests are simple to perform, and can detect influenza A and B in less than 11 minutes, at the point of care.
CLP: How does prompt testing of an individual with possible flu symptoms affect the spread of flu on a population level?
Hopps: Prompt testing at the point of care enables healthcare providers to confirm diagnoses and to take measures to stop further spread of the disease. As appropriate, such measures may include prophylactic therapy and isolation, depending on the setting. Additionally, such testing enables providers to give patients guidance on good respiratory etiquette and hand hygiene, and how to avoid close contact with people they know to be at increased risk of influenza-related complications. On average, patients are contagious for 7 days from the onset of symptoms.13
CLP: What advances in diagnostic testing for the flu do you hope to see in the future?
Hopps: In the future, I hope that more patients with flu-like symptoms are able to access fast, accurate testing easily in a variety of settings. By making flu testing more accessible, more patients will be able to seek treatment during the 48-hour window when antiviral drugs are most beneficial, and clinicians will be able to make informed treatment decisions for their patients, improving their treatment and preventing the development of antimicrobial resistance.
References
- Estimates of Influenza Vaccination Coverage among Adults: United States, 2017–2018 Flu Season [online]. Atlanta: Centers for Disease Control and Prevention, 2018. Available at: www.cdc.gov/flu/fluvaxview/coverage-1718estimates.htm. Accessed December 17, 2018.
- Goodie R. Tips for identifying the flu vs bacterial infection. Bellaire, Tex: St. Hope Foundation, 2017. Available at: https://offeringhope.org/tips-identifying-flu. Accessed December 18, 2018.
- Flu Symptoms and Complications [online]. Atlanta: Centers for Disease Control and Prevention, 2018. Available at: www.cdc.gov/flu/consumer/symptoms.htm. Accessed December 18, 2018.
- The Flu: A Guide for Parents. Atlanta: Centers for Disease Control and Prevention, 2018. Available at: www.cdc.gov/flu/pdf/freeresources/family/flu-guide-for-parents-2018.pdf. Accessed December 18, 2018.
- Blaschke AJ, Shapiro DJ, Pavia AT, et al. A national study of the impact of rapid influenza testing on clinical care in the emergency department. J Pediatric Infect Dis Soc. 2013;3(2):112–118; doi: 10.1093/jpids/pit071.
- Tanei M, Yokokawa H, Murai K, et al. Factors influencing the diagnostic accuracy of the rapid influenza antigen detection test (RIADT): a cross-sectional study. BMJ Open. 2014;4(1):e003885; doi: 10.1136/bmjopen-2013-003885.
- Linder JA. Editorial commentary: antibiotics for treatment of acute respiratory tract infections: decreasing benefit, increasing risk, and the irrelevance of antimicrobial resistance. Clin Infect Dis. 2008;47(6):744–746; doi: 10.1086/591149.
- Hicks LA, Bartoces MG, Roberts RM, et al. US outpatient antibiotic prescribing variation according to geography, patient population, and provider specialty in 2011. Clin Infect Dis. 2015;60(9):1308–1316; doi: 10.1093/cid/civ076.
- Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010–2011. JAMA. 2016;315(17):1864–1873; doi: 10.1001/jama.2016.4151.
- Antibiotic/Antimicrobial Resistance (AR/AMR). Atlanta: Centers for Disease Control and Prevention, 2018. Available at: www.cdc.gov/drugresistance/index.html. Accessed November 30, 2018.
- Rapid Influenza Diagnostic Tests [online.] Atlanta: Centers for Disease Control and Prevention, 2017. Available at: www.cdc.gov/flu/professionals/diagnosis/clinician_guidance_ridt.htm. Accessed December 18, 2018.
- Meury S, Zeller S, Heininger U. Comparison of clinical characteristics of influenza and respiratory syncytial virus infection in hospitalized children and adolescents. Eur J Pediatr. 2004;163(7):369–363.
- H1N1 Flu: Interim Guidance on Infection Control Measures for 2009; H1N1 Influenza in Healthcare Settings, including Protection of Healthcare Personnel [online]. Atlanta: Centers for Disease Control and Prevention, 2010. Available at: www.cdc.gov/h1n1flu/guidelines_infection_control.htm. Accessed December 18, 2018.
Steve Halasey is chief editor of CLP.


{kind=link}