
Experts discuss achievements, challenges, and what’s coming next
By Karen Appold
Moving out of basic science and research labs, genetic tests are increasingly being used in clinical laboratories to look for changes in an individual’s chromosomes or genes that lead to health problems or may increase the risk of developing a health problem. Chromosome tests include chromosome microarray tests—which use deoxyribonucleic acid (DNA) probes to identify tiny areas of gain or loss of genetic material. Such changes often involve more than one gene.
DNA testing looks for changes in the code of a gene that can alter how that gene functions. Whole-genome testing—made possible by recent advances in sequencing technologies—involves analyzing the code or sequence of nearly every gene for one individual simultaneously. More practically, whole-exome sequencing focuses attention on the 1% of an individual’s genome that codes for proteins—and is therefore most likely to have an effect on health.

David Flannery, MD, American College of Medical Genetics and Genomics
Genetic testing can now identify the causes of disorders whose basis was previously unknown, notes David Flannery, MD, FACMG, medical director at the American College of Medical Genetics and Genomics, Bethesda, Md. For one study reported in the New England Journal of Medicine, whole-exome sequencing was able to identify the causes of disorders in approximately 25% of 250 patients who had previously undergone other genetic tests that were inconclusive.1 In 62 of the 250 patients, 86 mutated genes were identified that the researchers believed caused the patients’ disorders.
WHY IT’S A GAME CHANGER

Jim Evans, MD, PhD, University of North Carolina at Chapel Hill
“Genetic testing is being pursued so widely because new technology has made it affordable,” says Jim Evans, MD, PhD, Bryson distinguished professor of genetics and medicine at the University of North Carolina at Chapel Hill, and editor in chief of Genetics in Medicine.
Another driver is the fact that the technology can be used to perform noninvasive prenatal testing, in which fetal DNA can be analyzed via the mother’s blood for conditions such as trisomy 21. “This is rapidly becoming the standard of care in obstetrics,” Evans reports.
In addition, genetic testing is being used to guide personalized medical treatments, including cancer treatment. “We now have the capability to identify and understand rare diseases, which has led to better knowledge of common diseases and better treatments, screening, and interventions,” says Howard M. Saal, MD, professor of pediatrics at the University of Cincinnati College of Medicine, and director of clinical genetics at the Cincinnati Children’s Hospital Medical Center. “Genetic testing has also led to increased understanding of many disorders, such as reaction to trauma, the specific mutations that cause cancers, how cancers develop resistance to chemotherapy, and how immune systems function. Few medical conditions have no genetic influence at some level.”
Nevertheless, genetic testing itself remains expensive. The cost isn’t just for the sequencing (which is declining in price). Rather, the analysis of the vast amounts of data that are generated is incredibly complex and daunting. “Thus, implementation of this new technology isn’t cheap, and third-party payors are understandably concerned,” says Evans.
“Many payors, especially governmental payors such as Medicare, some state Medicaid programs, and Tricare, have decided not to cover the majority of available genetic tests,” says Flannery.
GENETIC TESTING FOR CANCER AND BEYOND

Jeremy Stuart, ScD, MPH, Selah Genomics
One goal of newly developed tests is to overcome clinical challenges. In some cases, for instance, the standard of care may call for multiple tests to be performed—a difficult achievement when the quantity of biopsy material is limited. “More assays are being designed to use very small amounts of biopsy material while producing comprehensive test results,” says Jeremy Stuart, ScD, MPH, vice president of genomic services at Selah Genomics (an EKF Diagnostics Company), Greenville, SC. “This produces faster results and reduces the need for repeat biopsies.”
Another challenge is the heterogeneity of tumor samples, which can make it difficult to distinguish tumor from normal sample and get unambiguous results, reports Kim Caple, vice president of global clinical marketing at Affymetrix Inc, Santa Clara, Calif.
In the past year, technological advances and the pace of clinical trials have accelerated dramatically. For example, next-generation sequencing (NGS) techniques can enable the identification of somatic variants across multiple cancer-related genes at once, says Stuart.

Paul W. Dempsey, PhD, Cynvenio Biosystems
In addition, according to Paul W. Dempsey, PhD, chief scientific officer at Cynvenio Biosystems Inc, Westlake Village, Calif, cancer-related genetic information can now be obtained from cells and cell-free DNA recovered from a simple blood sample.
Scientists have also found a new class of tumor—copy-number alteration driven (C-class)—in addition to the previously known mutation-driven (M-class) tumor, Caple notes.
Along the way, the biggest obstacle that clinicians and laboratorians encounter is the need to continually stay at the forefront of developments. “Innovation in terms of diagnostic testing has been very rapid, and professional guidelines are rapidly evolving to keep pace,” says Scott Gleason, vice president of investor relations at Myriad Genetics, Salt Lake City.
Beyond cancer, genetic testing is playing a significant role in many disciplines. In fact, NGS and gene association studies are being run in almost every major area of human disease. Some areas, such as the autoimmune and neuropsychiatric spaces, have incredible potential for high-value diagnostics to drive better patient outcomes and lower healthcare costs, Gleason reports.
Genetic testing can also assess the risk of certain inherited disorders, and predict an individual’s response to certain drugs, such as clopidogrel for cardiology patients. “These results can help physicians tailor a dose or opt for alternative therapies,” Stuart says.
In other cases, “preventive measures can be taken when a genetic susceptibility to a particular disease is identified at a younger age,” Stuart continues. For example, biomarkers for early-onset Alzheimer’s disease are being actively investigated. He expects genetic tests for early-onset Alzheimer’s to be available in the next 5 years.
According to Caple, reproductive health is another focal point of genetic testing. Areas of interest in this field range from carrier screening, to embryo screening for in vitro fertilization, to noninvasive pregnancy testing, and postnatal testing. Diagnosing postnatal development delay and intellectual disabilities also top the list.
PLATFORM OFFERINGS
Molecular diagnostics manufacturers are advancing technologies to automate processes. Here’s a look at some of the major trends in new instrument development.

The CytoScan Dx assay by Affymetrix is the only FDA-cleared whole-genome test for aiding in the diagnosis of intellectual disabilities and developmental delay. Photo courtesy Affymetrix Inc, Santa Clara, Calif.
Personalis’ ACE clinical exome test is a clinical diagnostic test for rare genetic syndromes that has been augmented in a number of ways to enhance diagnostic yield. In addition to standard exome coverage, it provides coverage of more than 7,000 biomedically important genes, and adds clinically interpretable content outside of the exome—such as regulatory regions important in disease. The test includes a novel genome-wide structural variant assay and has an enhanced bioinformatic pipeline to increase accuracy and diagnostic yield.
Cynvenio Biosystems’ LiquidBiopsy is a sample-preparation platform that extracts tumor cells from a blood sample and prepares a cell-based and cell-free-based template that enables NGS to be performed on platforms such as the Ion Torrent by Life Technologies, now a brand of Thermo Fisher Scientific. “It is the first validated platform that allows reliable recovery of these very rare cells and is deployed in a CLIA laboratory,” says Dempsey. The platform can be distributed to support centralized preparation of tumor-derived templates.
Myriad Genetics’ myRisk test offers a 25-gene panel consisting of well-validated oncogenes that lead patients to have a high predisposition risk for hereditary cancer. “We utilize multiple technologies in the testing process, including NGS, Sanger sequencing, and microarray-based tests for large rearrangements,” Gleason says.

Shoba Anantha, Luminex
Luminex’s genetic assays for CYP2D6 and CYP2C19 and its cystic fibrosis assays are all cleared by FDA for use on the company’s LX100/200 instrument. The assays utilize polymerase chain reaction and allele-specific primer extension reactions to detect the genotype of the samples, says Shoba Anantha, product manager for genetics global marketing at Luminex Corp, Austin, Tex. After run completion on the instrument, the software automatically calls the genotype of each sample with no additional data analysis requirement from the user.
Selah Genomics’ somatic tumor panel, called PrecisionPath, uses NGS and can identify somatic mutations across 50 cancer-related genes. When applicable, it provides an interpretive report for the oncologist that lists approved therapies and clinical trials related to the identified mutation. PrecisionPath was designed for formalin-fixed, paraffin-embedded tissue and can be performed using only a small biopsy specimen.
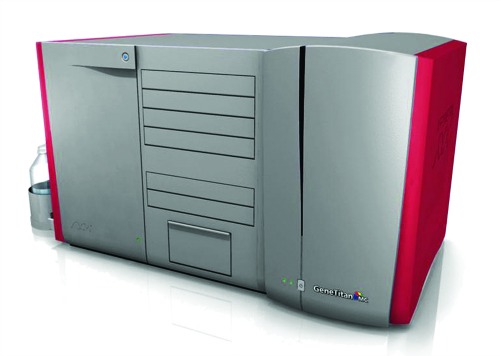
The GeneTitan multichannel instrument combines a hybridization oven, fluidics processing, and state-of-the art imaging device into a single benchtop instrument. Photo courtesy Affymetrix Inc, Santa Clara, Calif.
The GeneTitan multichannel instrument by Affymetrix automates array processing from target hybridization to data generation by combining a hybridization oven, fluidics processing, and a state-of-the-art imaging device into a single benchtop instrument. “Developed for use in genome-wide expression and genotyping studies, the instrument provides the highest throughput and laboratory productivity per technician by minimizing user intervention and allowing unattended overnight processing of large numbers of samples in parallel,” Caple says.
REACHING THE CLINICAL MARKET
Platform manufacturers are using a variety of strategies to penetrate the marketplace. “In terms of expanding exome sequencing, Personalis is focused on increasing its diagnostic yield, so that it makes sense to do exome sequencing earlier on in the process. Hopefully, this will prevent lengthy serial testing and difficult diagnostic odysseys,” says Adam Lowe, vice president of marketing for Personalis, Menlo Park, Calif.
Selah Genomics’ strategy for PrecisionPath is to seek Medicare and private-payor approval by demonstrating clinical utility, thereby gaining access to community oncologists.
WHAT THE FUTURE HOLDS
So is NGS headed away from direct clinical applications for individuals because of its heavy commitment to projects to sequence millions of genomes?
Evans doesn’t think so. “There are big projects, and they’re necessary to figure out how to interpret all the data. But individuals in the right clinical settings will have this done regularly.”

Douglas J. Moeller, MD, McKesson Health Solutions
“We are seeing NGS around cancer panels and cardiac panels, based on a number of genetic markers,” says Douglas J. Moeller, MD, medical director at McKesson Health Solutions, King of Prussia, Pa. “As NGS equipment becomes more widely available and affordable, we will continue to move in this direction of developing new panels that can help distinguish lower-risk patients from higher-risk patients.”
Looking ahead to the next 5 to 10 years, Saal expects clinical applications to expand to most individuals with rare diseases, as well as uncommon presentations of common disease. “Its utilization for cancer will increase dramatically, especially with sequencing of cancer genomes, leading to better cancer staging, and better and more targeted drugs as well as other therapies,” he says.

Roger D. Klein, MD, JD, Cleveland Clinic
Roger D. Klein, MD, JD, FCAP, medical director for molecular oncology at the Cleveland Clinic, and chair of the professional relations committee at the Association for Molecular Pathology, believes that mutation profiling using NGS will become the standard of care for many tumors in the coming years. “The cost of sequencing continues to decline exponentially, and it is rapidly becoming cost-effective to use a single NGS test to interrogate a tumor for mutations of known clinical significance rather than performing individual tests,” he says.
For tumors, exome sequencing is for the most part a research discovery tool, and will likely remain so for the foreseeable future. “Because cancer is inherently unstable genomically, and usefulness typically requires some change in treatment or management of the patient, addressing the enormous amount of data produced presents substantial challenges for clinical application,” says Klein.
By contrast, inherited disease exome sequencing will probably make continued inroads, first for more carefully selected patients with unexplained, apparently genetic disorders, and next, as the technology improves, as a substitute for disease-specific gene panels that are increasingly used in the diagnosis of inherited disorders, Klein adds.
In the distant future, most individuals may well have exome sequencing performed as routine testing for the management of most medical conditions. “Eventually, we may see exome sequencing performed as newborn screening,” says Saal. “However, before that occurs, many ethical questions and issues will need to be addressed. In addition, healthcare professionals and the general population will need widespread genetic education.”

Luminex’s xTAG genetic assays for CYP2D6 and CYP2C19, and the company’s cystic fibrosis assays, are all cleared by FDA for use on the Luminex LX100/200 instrument.
Whole-genome sequencing will probably require substantial technological improvements before it plays a serious role in medical practice, says Klein. However, one needs to separate the technical act of genotyping from the patient test. It may be that exome or genome testing will at some point become the primary means of acquiring genotyping data. At that point, the actual patient test would become an informatics exercise of selecting the specific data to unmask and evaluate in an individual patient.
On a related topic, says Klein, if FDA’s move to regulate laboratory-developed tests comes to fruition, it could have major adverse effects on patient access to genetic testing. “Oncology testing using next-generation sequencing is almost exclusively laboratory developed, and components of it have the same intended use as FDA-approved tests.”
Regulating such testing, says Klein, “would put a halt to much of this testing because most laboratories could not afford to go through a regulatory process in order to perform it. Importantly, the reimbursable components of NGS testing would need to be performed using alternative FDA-approved tests, eliminating the already scarce sources of payment for the testing.”
Experts say that the promise and future of genetic testing looks very bright. There have been some bumps along the way, and there will no doubt be more in the future. The ongoing struggle to balance high costs against low reimbursement rates remains a key obstacle to advances in the field. But given the benefits of genetic testing that have already become apparent, say the experts, growth of the field is certain to continue and gain momentum as the 21st century moves onward.
Karen Appold is a contributing writer for CLP. For further information, contact chief editor Steve Halasey via [email protected].
REFERENCE
1. Yang Y, Muzny D, Reid JG, et al. Clinical whole-exome sequencing for the diagnosis of mendelian disorders. N Engl J Med. 2013;369:1502–1511; doi: 10.1056/NEJMoa1306555.




{kind=link}