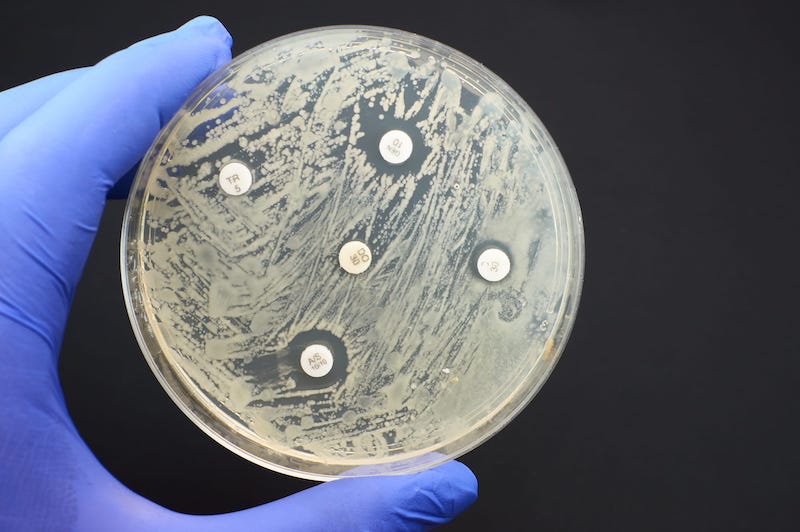
There were an estimated 4.95 million deaths associated with Antimicrobial resistance (AMR) in 2019, including 1.27 million deaths attributable to bacterial AMR, according to a study detailing comprehensive estimates of AMR burden.
Antimicrobial resistance (AMR) poses a major threat to human health around the world, according to the study Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis published in The Lancet.
AMR is a leading cause of death around the world, with the highest burdens in low-resource settings. At the regional level, the study estimated the all-age death rate attributable to resistance to be highest in western sub-Saharan Africa, at 27.3 deaths per 100,000, and lowest in Australasia, at 6.5 deaths per 100,000.
Lower respiratory infections accounted for more than 1.5 million deaths associated with resistance in 2019, making it the most burdensome infectious syndrome. The six leading pathogens for deaths associated with resistance—Escherichia coli, followed by Staphylococcus aureus, Klebsiella pneumoniae, Streptococcus pneumoniae, Acinetobacter baumannii, and Pseudomonas aeruginosa—were responsible for 929,000 deaths attributable to AMR and 3.57 million deaths associated with AMR in 2019.
One pathogen–drug combination, meticillin-resistant S aureus, caused more than 100,000 deaths attributable to AMR in 2019, while six more each caused 50,000–100,000 deaths: multidrug-resistant excluding extensively drug-resistant tuberculosis, third-generation cephalosporin-resistant E coli, carbapenem-resistant A baumannii, fluoroquinolone-resistant E coli, carbapenem-resistant K pneumoniae, and third-generation cephalosporin-resistant K pneumoniae.
The study estimated deaths and disability-adjusted life-years attributable to and associated with bacterial AMR for 23 pathogens and 88 pathogen–drug combinations in 204 countries and territories in 2019.
Data was obtained from systematic literature reviews, hospital systems, surveillance systems, and other sources, covering 471 million individual records or isolates and 7,585 study-location-years.
Researchers used predictive statistical modelling to produce estimates of AMR burden for all locations, including for locations with no data. The approach can be divided into five broad components: number of deaths where infection played a role, proportion of infectious deaths attributable to a given infectious syndrome; proportion of infectious syndrome deaths attributable to a given pathogen; the percentage of a given pathogen resistant to an antibiotic of interest; and the excess risk of death or duration of an infection associated with this resistance.
Understanding the burden of AMR and the leading pathogen–drug combinations contributing to it is crucial to making informed and location-specific policy decisions, particularly about infection prevention and control programs, access to essential antibiotics, and research and development of new vaccines and antibiotics.



{kind=link}