By Robert Schlaberg, MD, MPH
Certain infectious syndromes with nonspecific symptoms and myriad possible causes can turn into a diagnostic odyssey for patients, clinicians, and laboratories. Pneumonia and other respiratory syndromes fall into this category, as do conditions such as encephalitis and meningitis.
In large proportions of such cases, even patients who are tested repeatedly never get a clear answer about the specific cause of their infection. But a new approach to lab testing is promising to improve diagnostic success rates in such situations.

Robert Schlaberg, MD, MPH, University of Utah School of Medicine and IDbyDNA.
‘Clinical metagenomics’ is based on the concept of unbiased testing—that is, using DNA or RNA sequencing together with advanced bioinformatics to interrogate a sample without imposing preconceived notions, instead of looking for a specific pathogen or set of pathogens considered likely culprits. By looking broadly at organisms found within a sample, clinical metagenomics can detect even rare causes, without requiring laboratorians to resort to large panels of tests for suspected pathogens, or to pursue sequential approaches when initial tests come back negative.
Clinical metagenomics is designed to complement, rather than replace, existing lab tests with utility for specific types of cases. For patients who can be served well with conventional tests, there may be no justification for adopting the unbiased approach. But for patients with more complex health situations—severely ill patients, immunocompromised patients, patients whose initial tests came back negative—clinical metagenomics may open the door to getting actionable results quickly enough to inform medical decisions.
The clinical metagenomics approach can also be applied as part of clinical trial selection processes, in order to provide better targeting of patients with the specific infection under investigation (For more information, see “Metagenomics for Clinical Trial Selection and Companion Diagnostics.“)
Challenging Infections
There are causes of infection that practically announce themselves because of the symptoms they manifest or because the pathogens are known to be in circulation. In such cases, it is a relatively straightforward task for a physician to develop a strong hypothesis about the cause of the infection, perhaps based on a patient’s recent travel history, diet, or exposure to other infected individuals.
But there are many other types of infections that thoroughly frustrate physicians, patients, and clinical labs. Scenarios of this type often involve nonspecific infections with overlapping symptoms that could be caused by myriad potential bacteria, fungi, parasites, or viruses, or even nonbiological sources such as environmental toxins.
Such infections are difficult to treat in a targeted manner because diagnostic answers are so elusive. For 60% of pneumonia cases, for example, no pathogenic cause of infection is ever found. And the same is true for a majority of encephalitis, meningitis, and sepsis cases.1–4 Small wonder: there are hundreds of pathogens that can give rise to pneumonia alone.
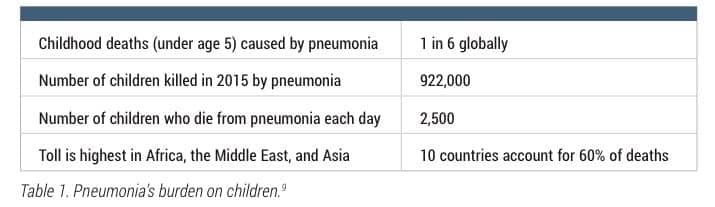
Table 1. Pneumonia’s burden on children.9
Thus operating more or less in the dark, healthcare teams default to empirical therapy, broad-spectrum antibiotics, and other approaches that cover a wide range of pathogens. Unfortunately, such responses are typically less effective than treatments that target a specific pathogen, and they also contribute to antibiotic overuse, which can worsen widespread resistance.
In part because of the lack of diagnostic information, each year in the United States there are more than 50,000 deaths from pneumonia and about 250,000 deaths from sepsis (Table 1).5,6 Globally, there were more than half a million deaths attributed to encephalitis or meningitis in 2015.7
One of the biggest obstacles to finding timely answers about such cases is the need to run separate clinical tests for each suspected pathogen or group of pathogens. Conventional testing may use cultures, immunoassays, or real-time polymerase chain reaction-based assays. But in cases where the potential causes of an illness are myriad, conducting a search one pathogen at a time can make the diagnostic process drag on interminably.
Unbiased Testing
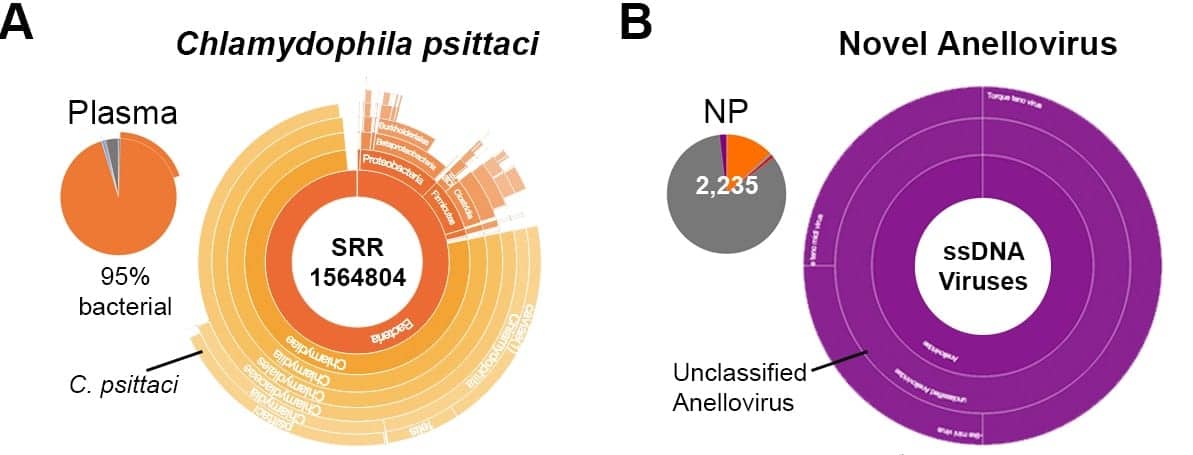
Figure 1. Examples of clinical pathogens identified through clinical metagenomic testing of patient samples: (a) analysis of a plasma sample from a patient suspected to have Ebola virus determined that the causative pathogen was actually Chlamydophila psittaci; (b) analysis of a nasopharyngeal swab led to the identification of a novel anellovirus as the causal agent. In both cases, traditional testing for likely culprits would not have been able to accurately identify the source of illness.
Metagenomics may be new to the clinic, but it has been used in research labs for years. The concept is to use DNA sequencing to scan quickly across an entire microbial population. Over the years, advances in DNA sequencing have made this method more affordable, while bioinformatics innovations have increased the speed, quality, and resolution of information that can be gleaned from this communitywide view.
Today, scientists have shown that partial or even complete genome sequences can be generated for all microbes in a specimen, even for complex microbial communities.8 The method has enabled scientists to generate novel data and make important discoveries about emerging pathogens, the interaction of microbial communities with plants and soil, and many other scientific areas.
It should come as no surprise, then, that scientists are eager to find ways to usher metagenomics into clinical use. From characterizing the biofilms in hospital drains to tracing the transmission path of a hospital-associated infection, there is significant benefit to be had from a higher-resolution method for assessing microbial communities and identifying specific members within them.
For clinical laboratorians, metagenomics offers a new way to think about diagnostic processes. In recent years, single-gene and single-organism tests have in many cases been replaced by panel-based tests that attempt to include all relevant genes or rational groupings of organisms, so as to streamline workup into a single test for faster results. Clinical metagenomics is the next step in this evolution: rather than looking for just one pathogen, or even among a few likely candidates, clinical metagenomics seeks to interrogate the sample without any preconceived notions or restrictions, and simply to determine what is in the sample.
Like its research-based cousin, clinical metagenomics relies on next-generation sequencing (NGS) of DNA and RNA, as well as advanced bioinformatics. Samples are shotgun sequenced, and all sequencing reads are then compared to vast genome databases. Millions of reads are matched to millions of reference sequences to identify all individual members of a sequenced population.
Because of its ‘sequence everything’ working model, clinical metagenomics is not limited to particular organism types the way most conventional tests are. Results can pinpoint viruses, bacteria, fungi, and parasites without having to make adjustments or establish any assumptions about the underlying pathogen. This advantage means that clinical metagenomics can identify pathogens that are difficult to culture, rare causes of infection, complex coinfection situations, and other medical states that have previously been challenging or even impossible to diagnose with existing clinical tests (Figure 1).
In Practice
Clinical metagenomics is not appropriate for all patient cases. At this time, clinical metagenomics is best used as a complement to traditional testing protocols. It can be applied in difficult cases after the usual suspects have been eliminated with conventional diagnostics, or as the first choice for high-risk patients, such as the severely ill or immunocompromised.
The method works best on samples from the infection site, in order to maximize the likelihood that any pathogens discovered are actually causing the infection, rather than harmlessly colonizing the patient. And because it sequences everything, the workflow takes 1 to 2 days to complete. For straightforward medical cases where conventional testing delivers actionable answers in a short time frame, clinical metagenomics would not make sense.
When a metagenomics approach is used, it must be integrated with advanced data analysis tools capable of filtering out the many benign organisms detected as part of the natural human microbiota. Bioinformatics can be used to prioritize likely infection-causing candidates so that reports sent back to physicians include only the most clinically useful information.
For testing labs considering the adoption of clinical metagenomics, thought should be given to send-out versus in-house diagnostics. At the moment, there are no FDA-cleared, commercially available clinical metagenomics tests.
Laboratorians can opt to design and validate their own lab-developed tests, which could be based on existing next-generation sequencing workflows. Such tests will require appropriate quality control for laboratory workflows and use of the bioinformatics processes described above for identifying, filtering, and prioritizing organisms from the patient sample.
Alternatively, CLIA-certified reference laboratories that have already validated clinical metagenomics tests could serve other clinical labs through send-out testing.
Naturally, reimbursement is a key consideration for either in-house or send-out testing. For hospitalized patients, clinical metagenomics testing can be covered as part of the diagnosis-relating grouping (DRG) payment for treatment performed in an inpatient setting. For use in outpatient settings, it will take time for payors to issue their coverage decisions.
What’s Next?
As clinical metagenomics matures, it will likely become easier to implement as an in-house diagnostic option at many sequencing-savvy clinical laboratories. As that happens, it will also become available for a broader range of infectious diseases.
Today, laboratory-developed tests for clinical metagenomics are limited to respiratory infections and a small number of other conditions. But because clinical metagenomics could theoretically work for any type of infection, scientists anticipate that the approach will be implemented for more indications in the near future.
To be sure, rolling out clinical metagenomics will require the generation and analysis of data to understand how such tests compare to existing tests, how they influence patient management, and their effects on patient outcomes and overall healthcare costs. In the coming years, it will be important for the clinical community as a whole to conduct in-depth studies of metagenomic assays.
Still, it seems evident that the adoption of clinical metagenomic tests will enable healthcare teams to solve more complex cases and bring the benefits of precision medicine to the realm of infectious disease. Ultimately, delivering medically actionable diagnostic results for more infectious disease patients should improve health outcomes and lower overall costs by shortening hospital stays and avoiding unnecessary treatments.
Robert Schlaberg, MD, MPH, is an assistant professor of pathology at the University of Utah School of Medicine, and chief medical officer at IDbyDNA, Salt Lake City. For further information, contact CLP chief editor Steve Halasey via [email protected].
References
- Jain S, Self WH, Wunderink RG, et al. Community-acquired pneumonia requiring hospitalization among US adults. N Engl J Med. 2015;373(5):415–427; doi: 10.1056/NEJMoa1500245.
- Sheldon IM. Detection of pathogens in blood for diagnosis of sepsis and beyond. EBioMedicine. 2016;9:13–14; doi: 10.1016/j.ebiom.2016.06.030.
- Brown JR, Bharucha T, Breuer J. Encephalitis diagnosis using metagenomics: application of next-generation sequencing for undiagnosed cases. J Infect. 2018;76(3):225–240; doi: 10.1016/j.jinf.2017.12.014.
- Kennedy PGE, Quan PL, Lipkin WI. Viral encephalitis of unknown cause: current perspective and recent advances. Viruses. 2017;9(6):138; doi: 10.3390/v9060138.
- Pneumonia [online]. Atlanta: Centers for Disease Control and Prevention, 2017. Available at: www.cdc.gov/nchs/fastats/pneumonia.htm. Accessed May 14, 2018.
- Sepsis: data and reports [online]. Atlanta: Centers for Disease Control and Prevention, 2017. Available at: www.cdc.gov/sepsis/datareports/index.html. Accessed May 14, 2018.
- GBD 2015 mortality and causes of death collaborators: global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study, 2015. Lancet. 388(10053):1459–1544; doi: 10.1016/S0140-6736(16)31012-1.
- Bishara A, Moss EL, Kolmogorov M, et al. Culture-free generation of microbial genomes from human and marine microbiomes. bioRxiv. Preprint, February 11, 2018; doi: 10.1101/263939.
- Pneumonia: Deadliest Childhood Disease [infographic]. New York City: United Nations Children’s Fund, 2015. Available at: https://data.unicef.org/wp-content/uploads/2015/12/world-pneumonia-day-infographic_242.pdf. Accessed July 3, 2108.



{kind=link}