
Lack of symptoms and antibiotic resistance are big hurdles
By Gary Tufel
In the United States as well as globally, recent increases in the prevalence of sexually transmitted infections (STIs) and the sexually transmitted diseases (STDs) they cause have been well-documented (see “Staggering Statistics on Scope of STD Problem“).1,4,5 The threat of STIs, and the need to screen for their presence, is strong. Molecular diagnostics, including next-generation sequencing (NGS), offer the promise of testing methods that are both faster and more accurate at finding sexually transmitted infections and diseases. But STIs still present major and unique challenges for detection and treatment, in part because such infections and their diseases are often asymptomatic.
The problem is not going away. In fact, the opposite is true: it’s increasing, because of many new challenges, says Peter Leone, MD, professor of medicine at the University of North Carolina School of Medicine, and adjunct associate professor of epidemiology at UNC’s Gillings School of Global Public Health. Many who contract STIs never develop the related disease, even though they’re infected by it and can still transmit it, says Leone. Such asymptomatic infections present enormous diagnostic and treatment challenges, he says.

Edward W. Hook III, MD, University of Alabama.
Recognizing the importance of such asymptomatic infections, the healthcare community is more and more using the term “sexually transmitted infections” in preference to the older term, “sexually transmitted diseases,” says Edward Hook, MD, a professor of medicine and epidemiology at the University of Alabama, Birmingham, and director of the STD control program for the Jefferson County (Alabama) Department of Health. “That’s because these STIs do lots of damage—especially when asymptomatic, as they often are—so patients who don’t appear to have the disease can still transmit it to others, which makes labs’ jobs even more vital.”
People who have STDs may be asymptomatic and not know they are infected, which is why getting a diagnostic test is critical, adds John Frels, PhD, divisional vice president for diagnostic product development at Abbott.
“For example, the presentation of syphilis after infection is typically a painless sore that may be mistaken for a skin bump or ingrown hair, or may be located in an area where it is not easily visible. In secondary syphilis a rash appears, but it is not an ‘itchy’ rash, so an infected person may not think much of it. Some people who are infected with syphilis do not have symptoms for years, even though the disease progresses and they remain at risk for health problems if they are not treated,” Frels says.
Fortunately, he notes, STDs such as syphilis can be treated and even cured, which is why it is so important to get tested.2,3
The cost of such infections is enormous, both in dollars and lives, says Leone. “But the big concern, according to statistics from the Centers for Disease Control and Prevention (CDC) for 2014, is that we’re seeing the first increase in chlamydia, gonorrhea, and syphilis all at once. We had hoped that better control of HIV was going to lead to decreases in these diseases.”4
“STDs are a significant global health challenge and continue to pose a substantial burden on the United States,” agrees Matthew J. Binnicker, PhD, associate professor of laboratory medicine and pathology at the Mayo Clinic, Rochester, Minn. According to CDC estimates, he notes, there were approximately 20 million new STIs in 2014. The patient populations most affected are those aged 15–24 years (see “STDs Are on the Rise, Some at Alarming Rate“). Not only do STIs cause acute disease, they may also cause long-term health consequences, including infertility, congenital infections, and potentially loss of pregnancies. Common STIs and related diseases include chlamydia, gonorrhea, herpes simplex virus (HSV), human papillomavirus (HPV), syphilis, and trichomoniasis. Trichomoniasis is the most prevalent nonviral STD in the United States, affecting approximately 3.7 million persons, he says. It is estimated that STDs account for $15 billion to $20 billion per year in healthcare costs.4,5
STI INCREASES
“The general population thinks of STIs as being drips, sores, and rashes,” Hook says. If that were their full extent, they wouldn’t be so important, he says. But STIs also cause ectopic pregnancies as well as congenital and neonatal infections. In addition, says Hook, “every STI studied so far carries the risk of transmitting the HIV infection to those who are exposed.” And the consequences and costs of these infections continue to rise.
Trichomoniasis is one such growing STI problem, Leone says. It is transmitted by a parasite from an affected to a nonaffected sexual partner, but some doctors don’t consider trichomoniasis to be an STD. And although health providers are not required to report cases of trichomoniasis in most states, the prevalence of Trichomonas vaginalis infection is on a sharp upward trend, especially among women. Trichomoniasis causes increases in the likelihood of HIV, pelvic infections, and premature childbirth. It’s also unique in that its likelihood of occurrence among women increases with age, instead of decreasing with age as with chlamydia. Current testing for trichomoniasis requires a single vaginal swab, which can be tested by molecular diagnostics making use of nucleic acid amplification technologies.
Although the extent of its increasing prevalence isn’t known, another major area of increasing STIs is ocular syphilis, which can lead to blindness among women and people with HIV, says Leone. Also of concern is the growth of congenital syphilis. And some varieties of gonorrhea have morphed into multidrug-resistant strains, Leone adds, increasing concern over the rise of antibiotic resistance connected to common STIs.
ANTIBIOTIC RESISTANCE
The challenges of dealing with STIs are not made easier by the fact that a number of pathogens are now being discovered in strains that have acquired resistance to the antibiotics previously used to treat them.

Susan Dolan, RN, MS, CIC, Children’s Hospital Colorado.
According to CDC, nearly a third of antibiotics prescribed in doctors’ offices, emergency rooms, and hospital-based clinics in the United States are not needed. “Improving the use of antibiotics is a national and international priority to help prevent antibiotic resistance which would threaten our ability to treat even the simplest of infections,” says Susan Dolan, RN, MS, CIC, an epidemiologist at Children’s Hospital Colorado, and 2016 president of the Association for Professionals in Infection Control and Epidemiology (see “More Than 75% of STD-Negative Patients Receive Antibiotics“).6
Beth Bell, MD, MPH, Centers for Disease Control and Prevention.
Diagnosis is critical for success against antibiotic-resistant infectious diseases, and the need for public health testing is building, according to Beth P. Bell, MD, MPH, director of CDC’s National Center for Emerging and Zoonotic Infectious Diseases.7 “We need to act now,” says Bell. “Diagnosis is part of the public health system’s effort to conduct disease surveillance, track resistance, stop outbreaks and prevent infections, and improve treatment efforts. Microbes are constantly changing and, with antibiotic resistance, there’s a growing need for rapid and innovative tests to detect new resistance trends. Current tests take some time, and improving methods will help clinicians know which treatments to use and when. NGS will be vital in the effort to improve diagnostics,” says Bell.
Some bacteria and viruses develop antibiotic resistance very readily, while others do not. Among STIs and their related diseases, syphilis does not develop resistance easily, while some strains of gonorrhea have developed resistance to nearly every antibiotic developed to treat them. In fact, as long ago as 2007, the emergence of fluoroquinolone-resistant Neisseria gonorrhoeae prompted CDC to stop recommending fluoroquinolones for the treatment of gonorrhea.
But the drug development pipeline that once produced many new antibiotics has been slowed by the rise of antibiotic resistance. Consequently, only antibiotics in the class of cephalosporins are still considered effective against gonorrhea.
According to Leone, progress is being made to address the rise of resistance to antibiotics that are prescribed to treat gonorrhea. Nevertheless, as a result of increasing antibiotic resistance, treatment failures have occurred even among patients on certain cephalosporins (ie, cefixime). Because of this, a dual treatment strategy with ceftriaxone and azithromycin is recommended for the treatment of gonorrhea in the United States.
“The bugs are quite varied, and new testing, management, and treatment methods are needed through the development of new, more-effective lab techniques,” Hook says. He expects that the next generation of testing will be able to tell if a strain of gonorrhea is treatable and, if so, how to treat it. “We’re not there yet, but research is leading to this,” he says.
THE NEED TO SCREEN
According to the World Health Organization, the majority of those with STIs have no, or only mild, symptoms. But even without symptoms that might lead to a positive diagnosis, there is still a risk that an STI can be transmitted to a partner without the carrier’s knowledge.
Because such a lack of symptoms can cause STDs to go unrecognized, Binnicker explains, screening is essential to prevent the spread of disease. All individuals aged 13 to 64 should be tested for HIV at least once, he says, and anyone who practices unsafe sex or shares drug injection equipment should be screened for HIV at least once per year.
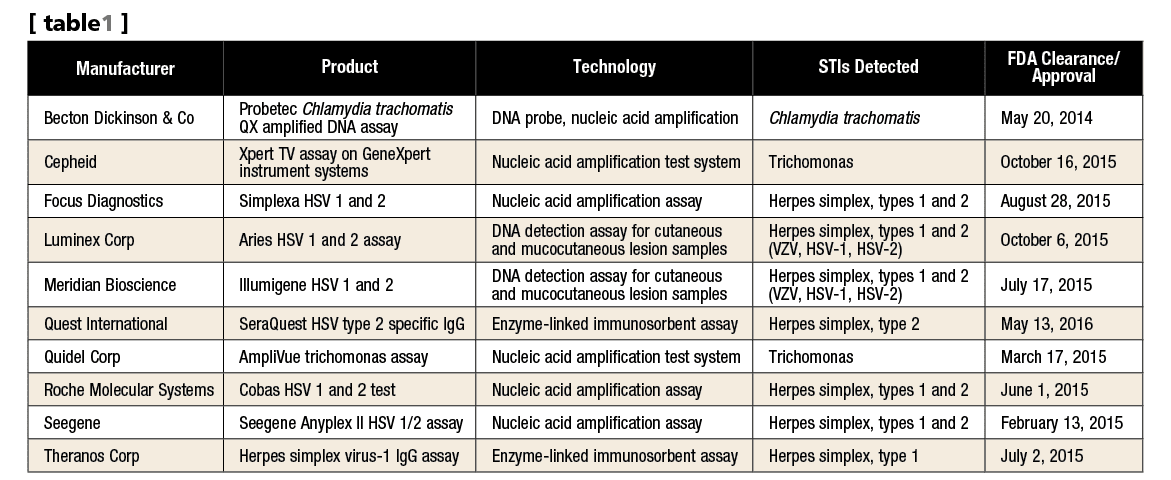
Table 1. A selection of FDA cleared and approved assays for sexually transmitted infections since 2014. Source: www.accessdata.fda.gov/scripts/cdrh/devicesatfda/index.cfm. Accessed June 20, 2016. Click to expand.
Annual screening for chlamydia and gonorrhea is recommended for sexually active women younger than 25 years of age as well as older women with high risk factors (eg, multiple sex partners). All pregnant women should be screened for chlamydia, hepatitis B, HIV, and syphilis early in pregnancy. And all sexually active gay, bisexual, and other men who have sex with men (MSM) should be screened at least once per year for chlamydia, gonorrhea, and syphilis.
“The clinical laboratory plays a key role in the diagnosis and management of STDs, but also in screening for STDs,” Binnicker says. “The choice of which lab test is preferred (ie, serology versus a molecular test) depends on the disease and the clinical situation. For example, screening for HIV is most commonly performed by a serology (antibody) test and, if the result is positive, the patient is then commonly tested by a molecular method (eg, real-time polymerase chain reaction [PCR]) to determine the patient’s viral load and monitor how he or she responds to therapy.
“Serology is also the recommended screening test for syphilis, since molecular tests may not be positive in the later stages of disease,” says Binnicker. “By contrast, molecular diagnostics are the recommended tests for screening and diagnosis of STDs such as chlamydia, gonorrhea, and trichomoniasis, because serologic tests for these infections are either unreliable or not available.”
Abbott, Abbott Park, Ill, recently received FDA clearance for a new syphilis test that will run on the company’s Architect family of immunoassay analyzers, the Architect Syphilis TP test. The test detects antibodies to Treponema pallidum (TP), the bacterium that leads to syphilis, says Abbott’s Frels.

John Frels, PhD, Abbott.
Upon infection with TP, the body develops an immune response that is directed against antigens specific to TP as well as antigens released during TP-mediated cellular damage, Frels says. Two types of tests have been developed as aids to diagnose syphilis, treponemal and nontreponemal. A positive treponemal test result indicates an acute, latent, or past infection with TP. Nontreponemal tests are especially valuable for monitoring disease activity and therapy response. To enhance diagnostic accuracy, says Frels, it is common practice for reactive test results of either a treponemal or nontreponemal test to be confirmed by a test of the complementary test type.
“The Architect Syphilis TP is a treponemal test that detects IgG and IgM antibodies to TP. Two different algorithms, which combine a treponemal with a nontreponemal test, are used as an aid in diagnosis of syphilis, says Frels. “The algorithm starting with the treponemal test is called a reverse screening algorithm, and has been implemented in laboratories due to the availability of automated treponemal tests.”
“The clinical lab is key for doctors being able to accurately diagnose STDs. The earlier a diagnosis can be made, the sooner treatment can begin, which may also help to lower the risk of spreading infections,” Frels notes.
Given the importance of reliable diagnosis of syphilis and other STDs, testing guidelines have been issued by different agencies such as the US Preventative Services Task Force, he says. For example, he points to several recommendations about STDs and syphilis testing made by CDC and FDA for healthcare professionals.8–10
MOLECULAR DIAGNOSTICS
“The clinical lab has a big role to play across the testing spectrum,” says Hook. And for STIs as for other diseases and conditions, molecular diagnostics represents a giant leap forward in testing.
“Molecular diagnostics offer very high specificity and greater sensitivity than cultures and other traditional testing methods,” says Hook. “It’s also easier to gather specimens. For instance, traditional testing methods for STDs often involved pelvic exams for women and swabbing up the penis for men. But because molecular testing is so forgiving and sensitive, urine samples are now taken from both men and women to test for STIs and STDs. It’s a revolution for lab testing with the potential for enormous good. Molecular testing is absolutely the gold standard,” he adds.
One of the first commercially available molecular tests for an STI was a PCR-based test for chlamydia, which was able to detect more infections and more diseases than was previously possible. Hook says that additional testing offers modest advantages, and that NGS will become important for determining what kind of infection is present. For instance, there are hundreds of HPV subtypes that may infect women, says Hook, but only a few can lead to cancer. Molecular diagnosis may be able to determine who will get cancer as a result of HPV infection.
Another sexually transmitted infection that has been affected by molecular testing is Trichomonas vaginalis, a parasite previously thought to be only found only in women, says Hook. But molecular testing has dramatically improved detection of the trichomonas parasite, and revealed that trichomoniasis can also be found in men.
“Given popular attention to and interest in sex, and how prevalent sexuality is in the media and in conversation, it’s obvious that we’ve done a poor job at providing information on STIs and STDs,” says Hook. “The United States has a much bigger problem with these diseases than other countries. We need to be better at testing and treating, and better at providing information on prevention,” he says.
Peter Leone, MD, University of North Carolina.
“It is the future,” says Leone of molecular diagnostics. “Because of their high sensitivity, they provide a high degree of certainty and specificity, along with low cost and ease of sample collection. Samples can be self-collected with a swab, fewer personnel are needed in the process, and there’s no special storage necessary.” The tests can be relatively expensive, he notes, but testing in volume brings the cost down. However gonorrhea, which lacks good markers to detect, presents a special challenge, but progress is being made in test development, he says.
Another challenge: HPV is carried by 80% of sexually active humans, Hook says, and a small percentage of those will get cancer because of it. Antibiotic resistance is also making treatment much more difficult.
And there are other factors. By definition, these sexually transmitted infections and diseases are largely diseases of the young, and those with them are, because of their youth, not very worried about it, says Hook. “Teenagers have the highest percentage of chlamydia and gonorrhea of any age group, and they’re not concerned about infertility at that age, or about the cervical cancer that can also result from these diseases 20 or 30 years later,” he says.
“We have not done a good job of controlling STIs or STDs. Sexual activity isn’t widely discussed with doctors, but it’s very prevalent in the media and in the culture,” says Hook.
“Gonorrhea can be present in the throat or in the rectum and unless those sites are screened, two-thirds of the cases can be present without the carrier’s knowledge. This makes screening vital, and nucleic acid amplification is a vital testing method,” says Leone.
One encouraging method is point-of-care testing—not a lab function per se, but a method that offers quicker results to young patients before they can spread the disease further, says Hook.
“We are trying to move the field toward more point-of-care testing,” agrees Leone. “With increasingly sensitive tests, lots of additional tests often aren’t needed. Doctors can screen, diagnose, and treat patients quickly, right on site. We already have point-of-care testing for hepatitis C, HIV, and syphilis. Newer, more-sensitive tests are beginning to offer these same advantages for other STIs,” Leone says.
There is also positive news for the use of patient self-screening methods, says Leone. “Self-screening test kits can be obtained via mail order, and test instructions direct patients how to collect their own samples,” he says. “Swabbing the vagina, penis, or rectum for STIs promises to ease the challenge of these asymptomatic infections. The test results still have to be validated by a clinical laboratory, but enlisting patients to initiate their own testing is an important step forward, because there are huge barriers to physician-ordered testing when the patient has no clinical symptoms.”
Leone emphasizes that molecular diagnostics is revolutionary in testing and in giving individuals control over testing via testing themselves. “Self testing eliminates the need for them to go to a clinic or a doctor to be tested. They can test in privacy and at home or go to a non-traditional provider.”
ADVANCING TO THE NEXT GENERATION
Recent advances have gone beyond molecular diagnostics in the diagnosis of STDs, especially in terms of the development of multiplex assays that can detect and differentiate several pathogens in a single test, Binnicker says. Examples of such next-generation techniques include assays that can detect Chlamydia trachomatis, Neisseria gonorrhoeae, and Trichomonas vaginalis all from a single sample.
He says another advance is in screening for HPV infection. New molecular tests allow for high-risk types of HPV to be detected, including specific genotyping of HPV-16 and HPV-18, which cause roughly 70% of cases of cervical cancer. Currently, there are no commercial NGS tests for the diagnosis of STDs, but this is an area of interest, and research is actively underway to develop these tests.
Leone says that NGS offers testing advances and advantages in detecting resistance patterns, but it’s more useful for large testing populations than for individuals. It may be able to detect the emergence of new organisms and STIs and to determine, using panels, whether flora are healthy or not.
TREATMENT STRATEGIES
Most STIs are asymptomatic, so screening and testing are very important, notes Leone. “For gonorrhea, there’s a two-drug therapy—ceftriaxone used with either azithromycin or doxycycline. But not every physician has access to these drugs, and many doctors therefore continue to treat gonorrhea with one drug. “The supply of these drugs needs to improve,” he says.
For syphilis, only Pfizer’s benzene penicillin is approved for treatment, says Leone. And for ocular syphilis and chlamydia there are also a limited number of drugs approved for use, he adds. “These drugs can be very cheap or very expensive, depending on their supply and availability,” says Leone. “There needs to be better oversight of manufacturers’ initiatives to produce more, because when a drug is only taken once, there’s less incentive for manufacturers to produce it.”
In order to identify and treat STIs and STDs while avoiding the complications they bring, testing must become more rigorous and comprehensive, says Hook. But the asymptomatic character of many such infections remains an obstacle.
“Those who are at risk and who are symptomatic and those who are asymptomatic must both be tested,” says Hook. “Young people with chlamydia and gonorrhea are most likely to receive effective treatment based on accurate testing,” he says, “but those who are asymptomatic present a bigger challenge for labs.”
Gary Tufel is a contributing writer for CLP. For further information, contact CLP chief editor Steve Halasey via [email protected].
REFERENCES
- Reported cases of sexually transmitted diseases on the rise, some at alarming rate [press release]. Atlanta: Centers for Disease Control and Prevention, CDC, 2015. Available at www.cdc.gov/nchhstp/newsroom/2015/std-surveillance-report-press-release.html.
- CDC fact sheet: syphilis & MSM (men who have sex with men) [online]. Atlanta: Centers for Disease Control and Prevention, 2016. Available at: www.cdc.gov/std/syphilis/stdfact-msm-syphilis.htm.
- CDC fact sheet: syphilis [online]. Atlanta: Centers for Disease Control and Prevention, 2016. Available at: www.cdc.gov/std/syphilis/stdfact-syphilis.htm.
- Sexually transmitted disease surveillance 2014. Atlanta: Centers for Disease Control and Prevention, CDC, 2015. Available at: www.cdc.gov/std/stats14/default.htm.
- CDC fact sheet: reported STDs in the United States; 2014 national data for chlamydia, gonorrhea, and syphilis [online]. Atlanta: Centers for Disease Control and Prevention, 2015. Available at www.cdc.gov/nchhstp/newsroom/docs/factsheets/std-trends-508.pdf
- More than 75% of STD-negative patients receive antibiotics [press release]. Charlotte, NC: Association for Professionals in Infection Control and Epidemiology, 2016. Available at: www.apic.org/for-media/news-releases/article?id=02864715-9310-453e-8924-58633d6cbc75. Accessed June 9, 2016.
- Bell BP. Infectious disease threats and response. Presented at Capitol Hill briefing (Washington, DC: AdvaMedDx, March 3, 2016).
- 2015 sexually transmitted diseases treatment guidelines: syphilis [online]. Atlanta: Centers for Disease Control and Prevention, 2015. Available at: www.cdc.gov/std/tg2015/syphilis.htm.
- Guidance for industry: recommendations for screening, testing, and management of blood donors and blood and blood components based on screening tests for syphilis. Silver Spring, Md: Center for Biologics Evaluation and Research, FDA, 2014. Available at: www.fda.gov/biologicsbloodvaccines/guidancecomplianceregulatoryinformation/guidances/blood/ucm411780.htm.
- Syphilis testing algorithms using treponemal tests for initial screening: four laboratories, New York City, 2005–2006. MMWR. 2008;57(32):872–875. Available at: www.cdc.gov/mmwr/preview/mmwrhtml/mm5732a2.htm.




{kind=link}
The chart of available assays was very incomplete. This is not the first time I have noticed listings of manufacturers of various analyzers/assays to be hit or miss as to what is actually available.