
The clinical lab community needs a shared vision for calculating the value of diagnostic testing.
By James J. Devlin, PhD
With the acceleration of new diagnostic and therapeutic innovations, healthcare stakeholders are increasingly using the methods of health economics and outcomes research (HEOR) to quantify the value of new products as they relate to clinical practice and reimbursement strategies. This trend is particularly evident in the area of precision medicine. Some new tests and therapies offer clearly evident value, potentially improving a clinical outcome at a low cost. For others, demonstrating value may require large-scale prospective trials or cost-effectiveness modeling.
Cost-effectiveness modeling is usually based on peer-reviewed publications that demonstrate the clinical effectiveness of a new test or therapy. To assess the cost of obtaining improved clinical effectiveness, the cost-effectiveness model evaluates both the improvement in effectiveness (often measured in life years gained) and the cost of obtaining these benefits. The cost of obtaining one additional year of life is referred to as the incremental cost-effectiveness ratio (ICER).
The use of such HEOR concepts has grown rapidly in recent years. When HEOR studies are carefully conducted, they can drive important decisions about access and coverage. To realize the promise of precision medicine, healthcare stakeholders must collaborate on an improved value assessment process that rewards innovation, improves efficiencies, accelerates clinical adoption, and facilitates use in patient care.
Researchers at Quest Diagnostics recently assessed the health and economic value of testing for seven genes known to confer increased risk of hereditary breast cancer. We found that testing for five additional genes, along with BRCA1/2 testing, provides health benefits at an acceptable economic cost, compared with BRCA1/2 testing alone.
Quantifying Value
Arguably, the most important word in healthcare right now is ‘value’—both clinical and economic. Healthcare innovations—diagnostic tests, therapies, and tests that guide the use of therapies—are coming to market rapidly, but across the spectrum of healthcare stakeholders, it is a challenge to quantify value as it applies to real-world clinical practice. And incomplete information about the value of such products has significant effects on their clinical adoption and reimbursement.

Figure 1. In the model used by Quest researchers to compare the seven-gene test strategy to the BRCA1/2 only test strategy, the number of life years gained and the incremental cost of each life year gained depend on the values assigned to multiple input parameters. To explore how changes in the testing assumptions might affect the results, a probabilistic sensitivity analysis was performed, recalculating the model 10,000 times, with different values for each of the input parameters being simultaneously and randomly drawn from reasonable probability distributions for each parameter. The figure shows that 95.7% of the 10,000 model results were under the diagonal line, indicating that 95.7% of the time, the life years gained cost less than $100,000 per life year.
In the diagnostic information services community, value is seen through two lenses. For clinicians, the value of a diagnostic is defined by its ability to provide actionable information associated with improved clinical outcomes, as measured by improved rates for curing disease, preventing adverse health-related events, or extending life.
But payors view value through a different lens. For them, the value of a diagnostic emphasizes the cost of each benefit it provides—not only in terms of direct costs, but also in terms of costs that will be either incurred or avoided during the episode of care that is delivered downstream of the diagnostic testing.
Within the healthcare ecosystem, these seemingly dichotomous considerations must coexist. For many tests and therapies, costs and outcomes align: if inserting a test into a pathway improves a clinical outcome at a low cost, the test obviously has value. But for many other tests and therapies, ‘value’ is a term that requires context. Payors must establish policies that enable them to assign value to tests that fall into a gray area—for example, a test that can recommend a treatment known to extend life, but by very little; or a test with a comparatively high cost for a condition that is very rare.
Payors’ conundrum extends beyond diagnostics: without utilizing laboratory tools that can dictate whether a particular therapy may be effective, payors can find themselves equally challenged to assign value to the therapy itself.
This article examines how HEOR concepts and methods help to quantify the clinical and economic value of laboratory services and related therapies, so that payors can formulate access and coverage determinations for those products. While HEOR currently offers a framework for making such determinations, analyses that arrive at the quality-adjusted life years (QALYs) and incremental cost-effectiveness ratios (ICERs) resulting from the use of a test or therapy are performed from a specific perspective; for example, from that of a payor. As such, they do not necessarily fully integrate the value of certain societal, ethical, and individual factors that would be important to those with a different perspective—for example, patients and caregivers—in precision medicine initiatives. (For more information, see “QALYs and ICERs: An Overview.”)
Precision Medicine Complicates the ‘Value’ Paradigm
One of the barriers to assigning value is the differing criteria by which health plans and payors evaluate new diagnostics or therapies for reimbursement. While they may take their cues based on rate-setting by the Centers for Medicare & Medicaid Services (CMS) or Medicare contractors such as Palmetto GBA, most third-party payors have their own methods for assessing economic value and appropriate reimbursement level. These processes evaluate a myriad of factors, including the guidelines of medical specialty societies, clinical validity, comparative effectiveness and, increasingly, economic benefit.
Similar but ultimately distinct processes that payors may use to assess the value of new products and services may function adequately when only a handful of major FDA-approved drugs or diagnostics are brought to market each year. But in today’s emerging era of precision medicine, diagnostic and drug developers are increasingly focused on companion diagnostics and highly targeted treatments that apply only to niche populations, making their value even more challenging to quantify.
Without large-scale biomedical information datasets that further our understanding of disease and the outcomes of targeted interventions—data that are aggregated by the diagnostic information services community—individual payors may lack the information they need to make informed value assessments and coverage decisions, let alone to align those determinations with those of others in the healthcare payor community. Such systemic weaknesses contribute to a fragmented system in which value remains unquantified and innovation unrewarded. And without adequate reimbursement, clinical uptake may be stymied.
Multiplexing for Value
A recently published study offers the opportunity to explore how the ‘value factors’ of QALYs and ICERs relate to testing and outcomes determinations.1
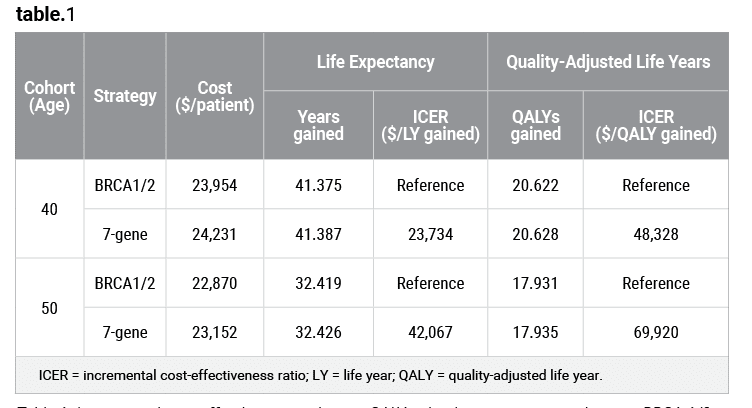
Table 1. Incremental cost-effectiveness ratios per QALY gained, seven-gene panel versus BRCA1/2 testing alone. Click to expand.
As a leader in oncology and women’s health, Quest Diagnostics sought to better understand the potential health and economic value of genetic testing for women at increased risk of hereditary breast cancer. Specifically, we investigated whether testing for five genes beyond the well-established BRCA1 and BRCA2 genes associated with heightened risk of breast cancer would confer health or economic value.
Our team of researchers developed a decision analytic (Markov) model for two hypothetical cohorts of 40-year-old and 50-year-old asymptomatic women with a family history of breast or ovarian cancer or other hereditary syndromes. The model compared two strategies for detecting pathogenic genetic variants and using the test results to select appropriate breast cancer risk reduction: the usual care strategy, which tests for variants in the BRCA1 and BRCA2 genes (BRCA1/2 testing); and a multigene strategy, which tests for variants in the BRCA1, BRCA2, CDH1, PALB2, PTEN, STK11, and TP53 genes (seven-gene testing).
We found that the hypothetical cohorts of 40- and 50-year-old women who underwent genetic testing with the seven-gene panel—followed by risk-reduction procedures as recommended by National Comprehensive Cancer Network guidelines—would see incremental cost-effectiveness ratios (ICERs) of $23,734 and $42,067 per life-year gained, respectively, when compared to BRCA1/2 testing alone (see Table 1).
To explore how changes in the testing assumptions might affect the results, a probabilistic sensitivity analysis found that the seven-gene test strategy cost less than $100,000 per QALY gained in 95.7% of the trials for the 50-year-old cohort (see Figure 1). This calculation suggests that the seven-gene test strategy would be cost-effective according to World Health Organization thresholds for the cost-effectiveness of interventions. It also compares favorably with annual screening for high-risk women via magnetic resonance imaging (MRI), which has an estimated ICER of $179,600.
In sum, the seven-gene strategy provides greater health and economic benefits than BRCA1/2 testing alone.
Our team at Quest Diagnostics has also conducted research that examined the cost-effectiveness of laboratory testing to aid oncology treatment selection.2 In this work, we sought to determine whether a next-generation sequencing (NGS) panel of 34 cancer-associated genes would cost-effectively aid in treatment selection for patients with metastatic melanoma, compared with a single-site BRAF V600 mutation test (see Figure 2).

Table 2. Incremental cost-effectiveness ratios per QALY gained, single-site mutation test versus gene sequencing panel. Click to expand.
In that study, we found that the gene sequencing panel strategy resulted in a cost of $120,022 and an increase of 0.721 QALYs per patient, while the single-site mutation test strategy resulted in a cost of $128,965 and an increase of 0.704 QALYs (see Table 2). Thus the key finding, from a US payor perspective, was that using an NGS panel of 34 cancer-associated genes to guide selection of first-line targeted treatment for metastatic melanoma could reduce medical costs and increase the patient’s quality and length of life, when compared with using a single-site mutation test.
Limitations of QALYs and ICERs
QALYs and ICERs are broadly accepted metrics that can be used to compare the relative value of healthcare interventions. Nevertheless, many factors that influence the value of such interventions cannot be adequately reflected by QALYs and ICERs alone. (For more information, see “More is not Necessarily Better.”)
For instance, HEOR studies are not intended to account for or assign a value metric to psychological or societal factors that may affect patients, such as their anguish or relief over knowing whether an effective treatment may be available for their disease—however remote its chances of success. Nor do such studies attempt to negotiate the ethical conundrums involved in impartially assigning value to the life and health of an individual, without considering any factors specific to that individual. While the selection and effectiveness of a particular cancer therapy often depend on the type of gene mutations occurring in the cancer tumor, for example, mutations vary for each individual and can even change during the course of treatment, which complicates the development of cost-effectiveness models.
Additionally, regulatory considerations, market competition (or lack thereof), and related cost considerations can make it difficult to include correct future pricing in the model.
Improving the HEOR Model in Diagnostics
On the whole, the healthcare community is just beginning to do the work that will be needed to realize the promise of precision medicine in clinical practice. To improve on the current HEOR model for determining the value of diagnostics, the diagnostic information services and health plan communities should work together more closely—and much earlier—to develop a standardized, evidence-based approach.
As a first step, test developers and payors should find ways to collaborate earlier on a shared vision of methods for calculating the value of diagnostic testing. In most other sectors of the economy, companies that are introducing products to the market usually begin with some understanding of what financial value the market will place on those products. In a similar fashion, diagnostic service providers should work with their prospective buyers to understand how to value their offerings before introducing them to the market. However, such early collaboration is often complicated by the fact that the buyer (the payor) is not the person (the patient) who receives the benefit.

Figure 2. A Quest Diagnostics scientist conducts next-generation sequencing (NGS) at the company’s San Juan Capistrano, Calif, high-complexity laboratory. Quest’s broad NGS offerings include IBM Watson Genomics from Quest Diagnostics, OncoVantage, and other diagnostic tests.
The same need for early collaboration applies to the relations between test developers and regulators, including the Clinical Laboratory Improvement Advisory Committee of the US Centers for Disease Control and Prevention, FDA, and bodies that certify product compliance with the European Union’s directive for in vitro diagnostics. Separately and together, such agencies are responsible for reviewing new diagnostic products, authorizing their entry to market, and ensuring that testing is carried out in accord with the regulations that apply to clinical laboratories.
While consistency in reimbursement evaluation and coverage decisions reduces inefficiency and uncertainty, there is a downside. Sometimes the successful introduction of a beneficial new diagnostic or therapy is based on a single payor deciding to offer coverage, which gives the innovation the chance it needs to fully demonstrate that it fills an unmet need. Therefore, modifications to the value assessment models should seek to avoid rigidity that could dissuade coverage by a single actor.
The lack of consistency and standardization has led to the emergence of differing approaches for making reimbursement and coverage determinations.
One such approach that has become a health plan mainstay is the ACCE model process for evaluating genetic tests, which is named for its key criteria—analytic validity; clinical validity; clinical utility; and associated ethical, legal, and social implications.3 While widely used, the process has not been revised to keep pace with innovations in test development, including the emergence of high-complexity genomic tests used for predictive testing.
More-promising models incorporate a collaborative approach. The Evidence Street pilot program of the Blue Cross Blue Shield Association is designed to create uniformity in the exchange of clinical evidence. It provides a route for companies to submit test data and see the information used to evaluate a device.4
Under an ideal approach, healthcare stakeholders—including the clinical laboratory community—will reach agreement on the baseline principles that are the underpinnings of value assessments, then use those principles to facilitate consistency across multiple organizations. Organizations such as the Personalized Medicine Coalition and, more recently, AdvaMedDx have proposed such cross-stakeholder approaches.5,6 Lessons from these approaches may support the development of future HEOR studies.
Conclusion
HEOR studies that measure the value of diagnostics and therapies in terms of QALYs gained and their associated ICERs imperfectly represent the totality of factors that contribute to the value of a healthcare intervention. Nevertheless, they remain a credible and widely used means of measuring the ‘value’ of new diagnostic services.
Greater engagement by diagnostic information service providers and other stakeholders—from health plans, to patients, to biopharmaceutical companies—in the task of defining and recognizing value will hasten innovation, improve efficiencies and, ultimately, help patients access the healthcare services they need.
James J. Devlin, PhD, is a senior science director and leads a chief medical officer analytics group at Quest Diagnostics. For further information, contact CLP chief editor Steve Halasey via [email protected].
References
- Li Y, Arellano AR, Bare LA, Bender RA, Strom CM, Devlin JJ. A multigene test could cost-effectively help extend life expectancy for women at risk of hereditary breast cancer. Value Health. 2017;20(4):547–555; doi: 10.1016/j.jval.2017.01.006.
- Li Y, Bare LA, Bender RA, et al. Cost-effectiveness of sequencing 34 cancer-associated genes as an aid for treatment selection in patients with metastatic melanoma. Mol Diagn Ther. 2015;19(3):169–177; doi: 10.1007/s40291-015-0140-9.
- ACCE model process of evaluating genetic tests [online]. Atlanta: Centers for Disease Control and Prevention, 2010. Available at: www.cdc.gov/genomics/gtesting/acce. Accessed May 15, 2017.
- Blue Cross Blue Shield Evidence Street [online]. Chicago: Blue Cross Blue Shield Association, 2017. Available at: https://app.evidencestreet.com. Accessed May 15, 2017.
- Pritchard DE, Moeckel F, Villa MS, Housman LT, McCarty CA, McLeod HL. Strategies for integrating personalized medicine into healthcare practice. Personalized Medicine. 2017;14(2):141–152; doi:10.2217/pme-2016-0064.
- A Framework for Comprehensive Assessment of the Value of Diagnostic Tests. Washington, DC: Deloitte Development, 2017. Available at: www.advamed.org/resource-center/framework-comprehensive-assessment-value-diagnostic-tests. Accessed May 31, 2017.

{kind=link}
I thought it was interesting that you said that the trend of needing to used HEOR is being increasingly more prevalent in the area of precision medicine. I think that the modern advances that are coming about in this century are amazing, and there are some great minds that are creating some of this stuff. I suppose that with all the new tech people need to be sure that their stockholders are happy with what they are paying for.