This is a companion article to the feature, “Liquid Biopsy Scores Immunotherapy Effectiveness.”
Non-small cell lung cancer (NSCLC) is the most common form of lung cancer, and is often diagnosed during the latter stages of the disease. Oncologists are therefore anxious to find the optimal treatment for their patients as quickly as possible.
Checkpoint inhibitors against programmed cell death protein 1 (PD-1) and programmed cell death protein 1 ligand (PD-L1) can be effective against NSCLC. But such drugs are approved only for a subset of patients who express high levels of PD-1 or PD-L1. This limitation has made it difficult to predict whether a patient will respond to anti-PD-1 or anti-PD-L1 treatment.1
PD-1 and PD-L1 expression are currently measured using immunohistochemistry (IHC) assays, which require that a tissue sample be procured via a biopsy. Not only is this method invasive, but IHC protocols and results are also highly variable among different laboratories, and can often produce ambiguous results.2,3 Furthermore, retesting tissue to resolve equivocal IHC results may require a second tissue biopsy, which puts patients at additional risk.
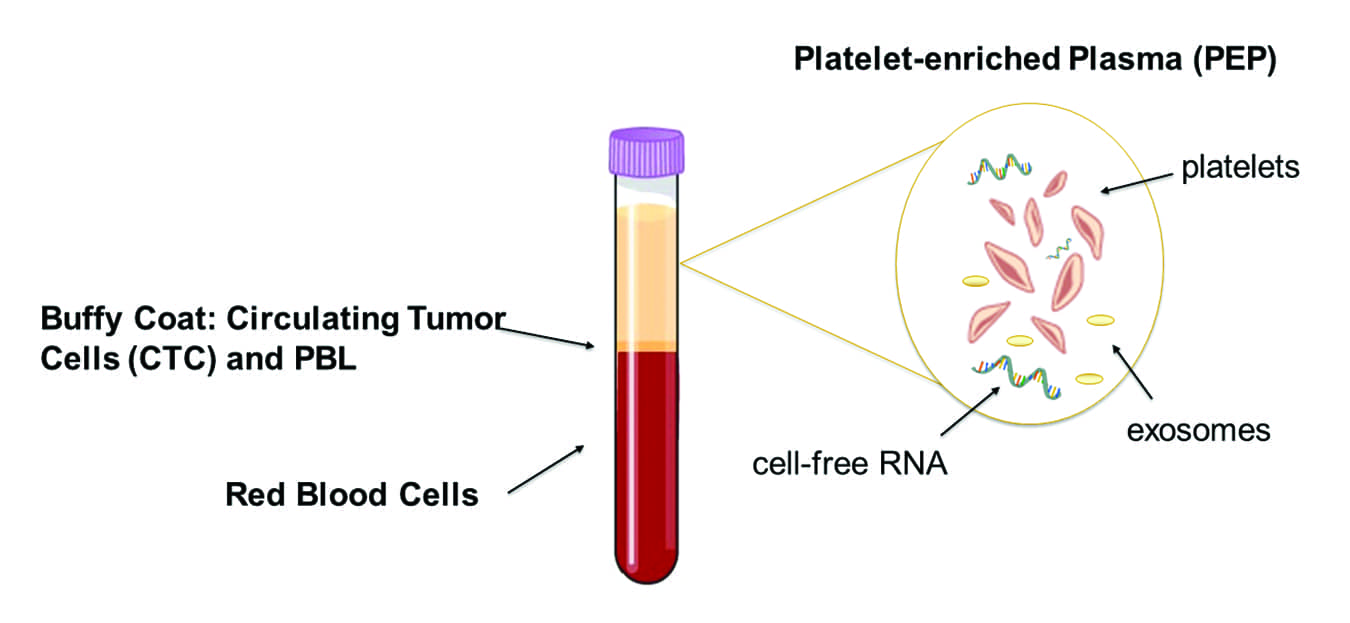
Figure 3. Isolation of platelet-enriched plasma (PEP). Whole blood collected into a Streck RNA blood collection tube is processed into PEP using low-speed centrifugation. RNA is then isolated, concentrated, and reverse-transcribed to cDNA.
A potential alternative to IHC for predicting patients’ response to anti-PD-L1 therapy is to use testing based on the droplet digital polymerase chain reaction (ddPCR) technique to detect changes in the mRNA expression levels in patients’ blood (Figure 3).
Earlier this year, Biodesix Inc, Boulder, Colo, presented preliminary study results demonstrating the feasibility of using ddPCR-based liquid biopsy testing to detect PD-L1 mRNA expression in plasma, potentially providing a supplementary method for objectively and reliably testing for PD-L1 expression. In the study, ddPCR detected PD-L1 mRNAs with a dynamic range of 32–138 copies from plasma.4 If validated, such a test could offer additional information to physicians who are evaluating an NSCLC patient’s eligibility for anti-PD-L1 therapy.
Since the ddPCR technique uses blood instead of tissue, testing is more easily repeated when additional results are needed. This is unlike invasive, tissue-based IHC assays, where repeat testing is not routine. Using ddPCR to detect differential mRNA expression could serve as a complement to ddPCR-based cell-free DNA tests, making it possible for oncologists to use noninvasive blood draws to detect biomarkers of actionable mutations as well as to monitor the effectiveness of immunotherapies.
References
- Gong J, Chehrazi-Raffle A, Reddi S, Salgia R. Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration trials and future considerations. J Immunother Cancer. 2018;6(1):8; doi: 10.1186/s40425-018-0316-z.
- Liu D, Wang S, Bindeman W. Clinical applications of PD-L1 bioassays for cancer immunotherapy. J Hematol Oncol. 2017;10(1):110; doi: 10.1186/s13045-017-0479-y.
- Hirsch FR, McElhinny A, Stanforth D, et al. PD-L1 immunohistochemistry assays for lung cancer: results from phase 1 of the Blueprint PD-L1 IHC assay comparison project. J Thorac Oncol. 2017;12(2):208–222; doi: 10.1016/j.jtho.2016.11.2228.
- Mellert HS, Jackson L, Pestano GA. Performance verification of a plasma-based PD-L1 test that reliably measures mRNA expression from patients with NCSLC. J Clin Oncol. 2018;36(5):156; doi: 10.1200/jco.2018.36.5_suppl.156.



