
FDA guidances raise issues of safety and efficacy for monitoring diabetic patients
By Steve Halasey
Diabetes is a well-known cause of serious health complications. People with diabetes are at significantly higher risk of such comorbidities as cardiovascular and peripheral vascular disease, neuropathy, kidney disease, blindness, and amputation.
The costs of caring for the diabetic population are staggering. A recent policy brief issued by the UCLA Center for Health Policy Research found that in 2011, nearly a third of California’s hospitalizations for patients aged 35 and over were for individuals with a diagnosis of diabetes. And while diabetes was almost never the cause of a patient’s hospitalization, “hospital stays for patients with diabetes cost nearly $2,200 more per stay than those for patients without diabetes, regardless of the patient’s primary diagnosis.”1
KEEPING TRACK
Laboratorians and nursing staff are among the first to feel the burden of hospitalized diabetics—including a sizable proportion of patients yet to be diagnosed with the disease. To forestall the development of further health complications, such patients need frequent monitoring of their glucose levels as well as heightened levels of care, adding to overall costs and demands on staff.
In the past, the expedient tool for keeping tabs on a patient’s blood glucose levels has been the well-worn point-of-care blood glucose meter. Offering speed, portability, and accuracy, such devices have become the mainstay of diabetes care in patient homes as well as in professional healthcare settings.
But no more.
After several years of wrangling with nagging issues related to the accuracy of meter readings when used for patients not previously diagnosed with diabetes, or for critically ill patients whose conditions might affect meter readings, FDA has recently proposed to create two distinct standards for professional-use and home-use glucose meters. Explaining the rationale for its proposed shift in policy, FDA wrote:
“Use of glucose monitoring devices in professional healthcare settings when they were cleared for lay use puts patients at increased risk. The performance of the devices was not evaluated in the intended use population, and the scientific and clinical issues may not have been adequately addressed for these uses. Therefore, where devices are intended for use in professional healthcare settings, distinct performance parameters should be met and sponsors should demonstrate substantial equivalence for that particular use.”2
To formalize the policy change, in January FDA issued two separate draft guidance documents, one for glucose monitors intended for prescription point-of-care use, the other for monitors intended for over-the-counter sale and personal use.2,3 Each document includes extensive instructions for the studies that manufacturers should conduct in order to demonstrate that their products meet the newly defined standards.
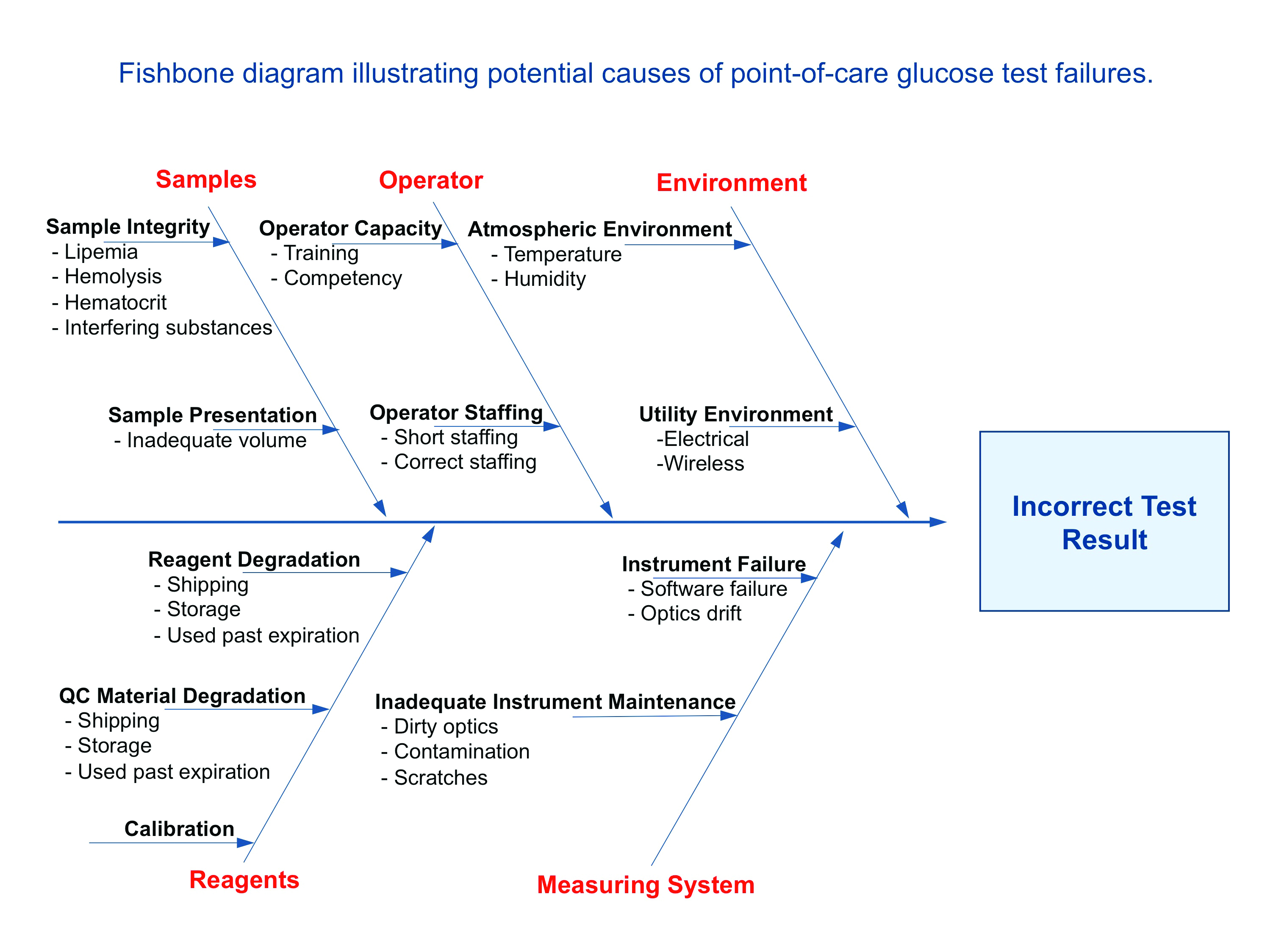
Diagram courtesy of St Elizabeth Medical Center
INCREASING THE LAB BURDEN
Not everyone has been thrilled with FDA’s newly proposed guidances. After a deliberate review of the proposals, in early May the American Association for Clinical Chemistry (AACC) came out against the idea of recategorizing professional-use blood glucose meters as moderate complexity devices.

James H. Nichols, PhD
“Although we support the agency’s objective, reclassifying prescription-use blood glucose monitors will add to the regulatory burden for healthcare providers by increasing their personnel documentation, proficiency testing, and method performance certification requirements under CLIA’88,” says James H. Nichols, PhD, medical director of clinical chemistry at Vanderbilt University Medical Center and chair of AACC’s government and regulatory affairs committee.
“We do not believe that this will improve patient outcomes,” Nichols says. “In fact, we are concerned that the opposite may occur if glucose meters are suddenly removed from critical care settings, where they are effectively used to measure and manage glucose levels, thus contributing to better patient outcomes.”
Sudden removal was no imaginary possibility. Just days after publication of FDA’s draft guidance documents, the New York State Department of Health issued a letter to its licensed labs in New York, instructing them to discontinue the use of blood glucose monitors in settings or populations not included in the intended use statements for those devices (see sidebar, page 22).
“The Centers for Medicare & Medicaid Services (CMS) have instructed us that the laboratory must be informed that in the event of such off-label use, the glucose meter defaults to high complexity and the laboratory must meet CLIA requirements for high complexity testing.”
In New York, the department continued, this would mean that only personnel licensed by the New York State Education Department would be eligible to perform the testing.
CONCLUSION
FDA has repeatedly emphasized that its guidance documents are meant to guide performance evaluation studies conducted by manufacturers in preparation for premarket submissions under the new policies. They are not intended for labs.
For labs needing to conduct validation studies in order to preserve the use of their existing monitors, the agency instead recommends procedures developed by the Clinical and Laboratory Standards Institute.4
But it remains to be seen whether labs can shoulder the additional burden of validating older monitors. The 120-day period for submitting comments on FDA’s draft guidances closed at the beginning of May, so now the ball is in the agency’s court.
For more information, see the sidebar, “Validation of the Accu-Chek Inform II for Critical Care Use.”
Steve Halasey is the chief editor of CLP.
References
1. Meng YY, Pickett MC, Babey SH, et al. Diabetes Tied to a Third of California Hospital Stays, Driving Health Care Costs Higher. Health Policy Brief. Los Angeles: UCLA Center for Health Policy Research, 2014.
2. Blood Glucose Monitoring Test Systems for Prescription Point-of-Care Use. Draft Guidance for Industry and Food and Drug Administration Staff. Rockville, MD: FDA, Center for Devices and Radiological Health, 2014; available at: www.fda.gov/downloads/medicaldevices/deviceregulationsndguidance/guidancedocuments/ucm380325.pdf. Accessed May 21, 2014.
3. Self-Monitoring Blood Glucose Test Systems for Over-the-Counter Use. Draft Guidance for Industry and Food and Drug Administration Staff. Rockville, MD: FDA, Center for Devices and Radiological Health, 2014; available at: www.fda.gov/downloads/medicaldevices/deviceregulationsndguidance/guidancedocuments/ucm380327.pdf. Accessed May 21, 2014.
4. Point-of-Care Blood Glucose Testing in Acute and Chronic Care Facilities; Approved Guideline. 3rd ed. CLSI Standard POCT12-A3. Wayne, Pa: Clinical and Laboratory Standards Institute, 2013.



{kind=link}