
New survey examines the causes of low STI testing rates among young women
Interview by Steve Halasey
Despite record high rates of new cases of sexually transmitted infections (STIs), young women who are sexually active often don’t talk to their clinicians about sex and STI risk, and many are not being tested for infection or disease as guidelines recommend, according to new research from Quest Diagnostics.1
The findings from a new survey suggest that lack of communication between clinicians and patients—and false beliefs about STI risk held by both groups—may contribute to STI prevalence.

Damian P. Alagia III, MD, FACOG, FACS, Quest Diagnostics.
The Quest survey examined the perceptions of young women aged 15 to 24; mothers of young women in this age group; and primary care, OB/GYN, and other specialty physicians regarding sexual activity, sexual health, and knowledge of and screening for STIs. The results of the 2017 survey were also compared to those of previous research by Quest in 2015 involving similar populations.
To find out more about Quest’s survey on STIs, CLP recently spoke with Damian P. Alagia III, MD, FACOG, FACS, medical director for women’s health at Quest Diagnostics.
CLP: In comparison to other periods, how serious is the current rise in the incidence of STIs?
Damian P. Alagia III, MD: It’s extremely disconcerting for a few reasons. First, over the past few years the rates of syphilis, chlamydia, and gonorrhea diagnoses have all been increasing. And they are increasing concurrently in a dramatic fashion; prior to 2014, we hadn’t seen such a concurrent increase since 2006. Syphilis was at a historic low in 2000, and gonorrhea hit an all-time low in 2009; but now both are increasing at double-digit rates.
Second, CDC incidence and prevalence estimates tell us that young people aged 15–24 years acquire half of all new STIs, and that one in four sexually active adolescent females has an STI.
And finally, rates are increasing even though we have medical guidelines that provide a screening framework for physicians, more accurate diagnostics to help identify infections in their early stages and, arguably, better access to care and treatment for infected individuals.
So we have to ask, why is that happening? Our research suggests two of the biggest barriers are education and communication. These are big challenges, but they are not insurmountable.
CLP: The Quest survey focused on young women aged 15 to 24. Are they at greater risk of acquiring an STI than other groups?
Alagia: Well, anyone who is sexually active is at risk of acquiring an STI. We wanted to understand some of the factors that might be contributing to the record rates of increase, especially among young women.
We also focused on young women because one of the ironies of many common STIs is that while they are equal opportunity diseases, with men and women diagnosed at roughly equal rates, their clinical manifestations are often different. Differences in human anatomy make it more challenging to recognize the symptoms of infection in women, and many infections go undiagnosed. As a result, women are much more likely to suffer such long-term health effects as pelvic inflammatory disease and infertility from diseases such as chlamydia and gonorrhea.
CLP: What did the Quest survey reveal about why young women are at greater risk of acquiring an STI?
Alagia: What we found is that young women don’t see themselves at risk—which unfortunately increases their risk. Only 4% of sexually active young women said they were at risk for chlamydia, and only 2% said they were at risk for gonorrhea. When you consider that only 39% of these women said they used a condom during their last sexual encounter, that’s a very worrisome disconnect between sexual activity, perceived risk, and actual risk.

Figure 1. Young women are uncomfortable, and not always truthful, in patient-physician communication about STIs.
Young women are also at greater risk because they are not comfortable talking to their clinicians about sex and STIs; and when they do, they might not always be truthful. About half of the sexually active young women in our survey reported that they do not want to bring up for discussion the topics of sex or STIs, and one in four admit that they often don’t tell the truth about their sexual history to their clinicians (Figure 1).
Moreover, they don’t ask to be screened: 62% say they don’t ask to be tested because they are not at risk; and about half say they don’t ask to be tested because they don’t have any symptoms. Such a lack of testing not only impedes treatment for infected individuals, it increases the potential for infection transmission to others.
And finally, young women appear to be at greater risk because of the discomfort of their own clinicians. About one quarter of primary care physicians said they were very uncomfortable discussing STI risks with their female patients. So how does that play out in clinical practice? If clinicians are uncomfortable, it’s less likely they are asking about testing. And the data seem to bear that out, if you consider that only half of the young women surveyed said their clinicians had asked them about STI testing.
CLP: What do current medical guidelines recommend with regard to STI screening?
Alagia: In terms of young women in the age group we surveyed, CDC guidelines recommend annual chlamydia and gonorrhea screening for all sexually active women younger than 25 years. Given our findings, I want to emphasize that all sexually active women should be screened regardless of other factors, such as number of sexual partners or lack of symptoms. Many STIs are asymptomatic.
In addition, all women aged 13–64 should be screened for HIV. And, for women seeking evaluation for STIs, the physician should also consider testing for herpes and HIV. Pregnant women should be tested for syphilis and HIV at their first prenatal visit. Medical guidelines also define certain circumstances in which women should be tested for trichomonas.
Finally, although cervical cancer guidelines are in the process of being modified, current guidelines recommend that women aged 21–29 should be screened by cytology for human papillomavirus every 3 years.
CLP: What did the Quest Survey reveal about actual rates of screening among young women?
Alagia: Only about half of young women report that their clinicians have asked if they want STI testing. And only one in four sexually active women have asked their healthcare professionals for an STI test.
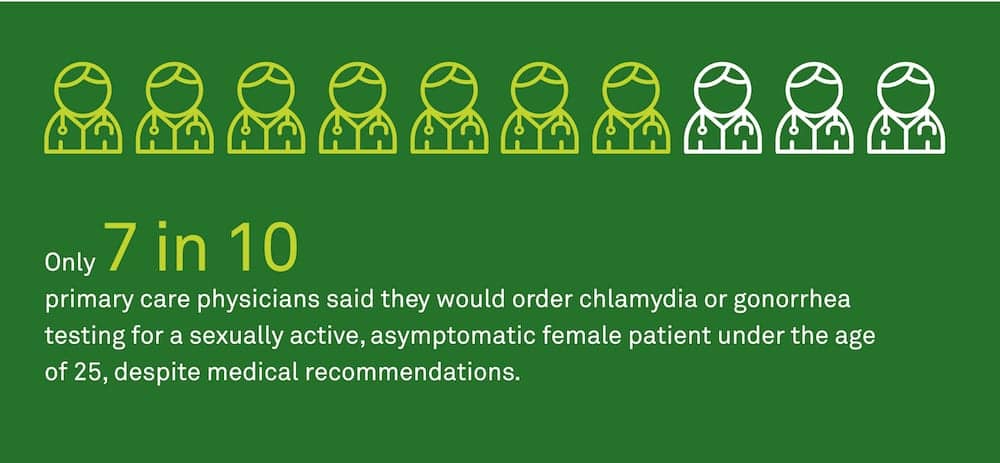
Figure 2. A quarter of physicians surveyed make testing decisions for asymptomatic young women based on the presence of symptoms.
We assumed physicians would report that they always screen according to guidelines. So we were surprised to find that only seven in 10 primary care physicians said they would order chlamydia or gonorrhea testing for a sexually active, asymptomatic female patient under the age of 25 (Figure 2).
CLP: Why are young women not being screened as the medical guidelines recommend?
Alagia: Most STDs are treatable if they are identified and treated at the earliest and most manageable stage. But it’s possible that physicians feel they will offend or cause discomfort for their young female patients by talking about STI risk and testing. It’s also possible that physicians feel those conversations aren’t appropriate with minors.
Nevertheless, it is important for physicians to engage their patients in meaningful and nonjudgmental conversations that focus on empowering women to take an active role in their own healthcare. Any discomfort that physicians might have should be alleviated by the knowledge that they are keeping their patients safe. The bottom line is that physicians must be proactive in these conversations.
CLP: How do healthcare professionals figure into this picture? Are clinicians educating young women and encouraging them to be tested?
Alagia: I think it’s a work in progress. Three in 10 physicians are not ordering screening tests for asymptomatic young women; but that means seven in 10 are doing so. We hope that these findings inform a dialogue around communication barriers, and that clinicians will revisit how they assess and care for young female patients—especially those who do not present with any symptoms of an STI.
Young women should also be encouraged to be completely honest with their healthcare teams, and to ask to be screened for STIs every year. When young women are empowered at an early age to ask questions about their health, to communicate honestly about their needs, and to request the screenings they deserve, the conversations will become much easier.
CLP: Are young women able to obtain accurate information about STIs from other sources, such as their parents, schools, or church groups? What did the survey reveal about the involvement of those sources?
Alagia: The messenger is very important—arguably just as important as the message. CDC and other organizations are doing a very good job at communicating the risks and effects of STIs, and the need for guidelines-recommended STI screening.
But when you’re young, you think you’re invincible. That’s when young people need their physicians and their parents—and for young women, especially their mothers—to guide them toward good healthcare decisionmaking. The vast majority of the young women surveyed said they primarily learned about STIs at school, in sex education or health classes. Only half reported that they learned about STIs from their clinicians, and only one quarter of young women mentioned they had learned about STIs from their mothers.
CLP: Quest conducted a similar survey about STIs in 2015. Were the responses of the recent survey significantly different in any areas?
Alagia: When we compared the two datasets, two findings stood out. First, more young women reported unprotected sex. In the recent survey, about 39% claim their partner used a condom the last time they had sex. In 2015, this number was 49%. That’s a very significant drop in reported condom use.
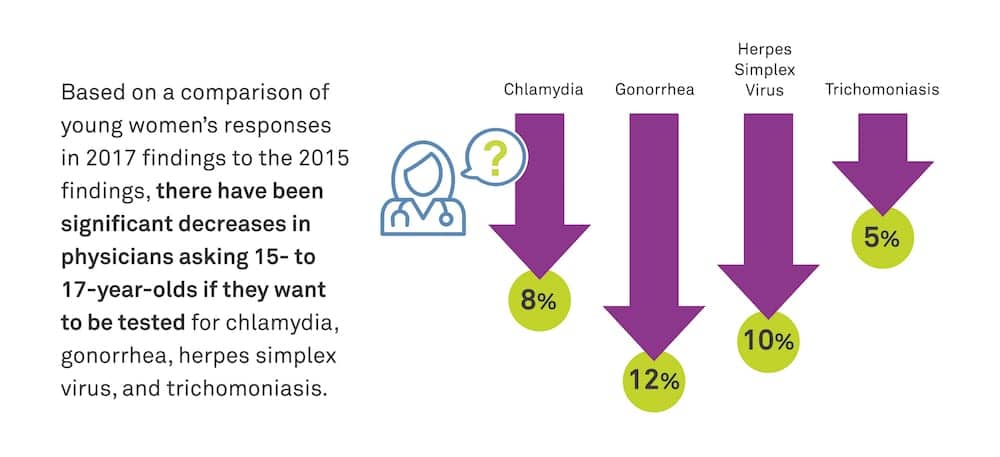
Figure 3. Physicians are currently less likely to discuss or offer STI screening to women aged 15–17 than in recent years, putting this group at the highest risk.
And there was a marked decline in screening among the youngest women, those 15–17 years of age. Based on a comparison of the 2015 and 2017 responses of sexually active women aged 15–17, STI testing by clinicians for chlamydia and gonorrhea has decreased by 9% and 11%, respectively (Figure 3).
Taken together, these two findings—decreased condom use and lower screening rates among the youngest women—are very disconcerting, because they suggest that the youngest women may be at the greatest risk of infection.
CLP: What changes can the healthcare community make to overcome the reduced rate of STI screening among young women?
Alagia: The most significant takeaway from our STI research is the importance of communication—particularly in patient-physician interactions—to ensure adherence to guideline-based care.
Physicians may feel they will offend or cause discomfort for their young female patients by talking about STI risk and testing. They may also feel that such conversations are not appropriate with minors. Still, the bottom line is that physicians and their office staff must be committed to having those conversations in a caring and nonjudgmental environment with young women and, in the case of minors, with a parent.
Healthcare practitioners need to stress to young women that the actions they recommend, including STI screening, are recommended because they care about their patients’ health. When that’s the foundation of healthcare delivery, everything else will fall into place.
CLP: What can laboratorians do to support these goals?
Alagia: In my opinion, laboratorians, with their incredible commitment to patient care and their critical thinking about testing, have made the most significant advances in removing barriers to STI testing. They should take well-deserved credit for developing and making available more convenient, highly sensitive tests than ever before, such as molecular diagnostics using nucleic acid amplification technologies.
Among young women in particular, a pelvic exam or uncomfortable testing is definitely a barrier to testing, so molecular diagnostics are particularly beneficial for clinical practice. And molecular diagnostics have higher sensitivity than traditional tests—approaching 95%—so clinicians can diagnose 50% more chlamydial infections.
Steve Halasey is chief editor of CLP.
Reference
- Young Women and STDs: Are Physicians Doing Enough to Empower their Patients and Protect their Health? A Survey of Young Women, Mothers, and Physicians about Sexually Transmitted Diseases (STDs) [online]. Secaucus, NJ: Quest Diagnostics, 2018. Available at: www.letstalkaboutstds.com. Accessed April 16, 2018.



{kind=link}