
An assessment of changing beneficiary access to laboratory services is essential
Interview by Steve Halasey
In the middle of February, laboratory accreditation organization COLA, Columbia, Md, sent a letter to the US Government Accountability Office (GAO) requesting an expansion of its recent report on the implementation of rate cuts to Medicare’s clinical laboratory fee schedule (CLFS).1
Specifically, COLA has asked GAO to address “the impact of the new payment methodology on Medicare beneficiary access to laboratory services,” which was not considered in GAO’s earlier report.2 At the same time, COLA offered to share with GAO the results of a nationwide 2017 study and 2018 survey of clinicians, which the organization conducted to understand the value of near-patient testing to patient care, and to evaluate the effects of current trends in reimbursement on access to laboratory testing.
“The 2017 summative evaluation study revealed valuable knowledge of how laboratory information supports physicians in the diagnosis, treatment, and care of their patients,” says John T. Daly, chief medical officer of COLA. “Several unique features of the study included in-depth interviews and a national physician practice survey to gather quantitative and qualitative data from practicing physicians who perform in-office testing across the United States. We have offered to share our preliminary data with GAO as a supplement to their published report.”
In the 2018 COLA follow-up survey, just over 56% of participants reported that further cuts in the CLFS will likely cause them to stop providing laboratory services. “We are deeply concerned about the impact of PAMA-related cuts on near-patient testing, especially in rural communities,” says Daly. “In some cases, near-patient testing in those communities saves lives.”
To find out more about COLA’s data on how labs are responding to reductions in CLFS pay rates, CLP recently spoke to John T. Daly, chief medical officer of COLA.
CLP: Why did GAO undertake its study of the new pay rates under Medicare’s clinical lab fee schedule (CLFS)?
John T. Daly, MD: When Congress enacted the new payment methodology through the Protecting Access to Medicare Act of 2014 (PAMA), the law directed GAO to conduct a comprehensive analysis of CMS’s implementation of the new payment rates for clinical diagnostic laboratory tests.
CLP: What were the objectives of the GAO study, and how was its scope assigned?
Daly: PAMA itself outlines 10 areas that GAO was to include in its analysis and report to Congress. For example, GAO was asked to analyze the rates paid by private payors for laboratory services furnished in various settings, including how payment rates compare across settings, the trends in payment rates over time, whether the new payment rates accurately reflect market prices, and the impact of the new payments on low-volume labs. Equally important, Congress directed GAO to evaluate the impact of the new payment rates on Medicare beneficiary access to laboratory services.
CLP: What were the key findings of the GAO report?
Daly: The centerpiece of the GAO report is the financial impact of PAMA on future expenditures in the federal Medicare program. GAO drew three main conclusions. First, that CMS did not collect all the data from all the laboratories required to report their private payor rates, but the extent of noncompliance was unclear. Second, when applying the first 10% payment reduction, rather than using the 2017 national limits on payments for each laboratory test as the baseline for making reductions, CMS should have used average allowable amounts. Finally, GAO predicted that if CMS “does not address the risks associated with unbundling payment rates for panel tests,” the new methodology could lead to billions in excess payments.1
CLP: Do those findings agree with COLA’s data about reimbursement trends for clinical laboratory testing?
Daly: There are a number of experts who can speak to private payor trends in reimbursement as well as billing and testing practices in the sector. COLA’s focus is on collecting data to better understand the value of near-patient testing related to diagnosis, treatment, avoiding more-expensive downstream costs, and how patients will be affected if laboratories in various care settings close their doors. I do know that GAO’s conclusions have been met with substantial criticism from the laboratory community.
CLP: What has been the nature of that lab community criticism of GAO’s findings?
Daly: There is a great deal of disappointment, and in some cases outrage, over the content of the report and GAO’s conclusions. Many have argued that GAO fundamentally misunderstood the real-world billing practices for laboratory reimbursement, and such misunderstandings led to “false claims that Medicare is overpaying clinical laboratories for panel tests.”3
CLP: Were there particular findings in the GAO report that led COLA to request an expanded version?
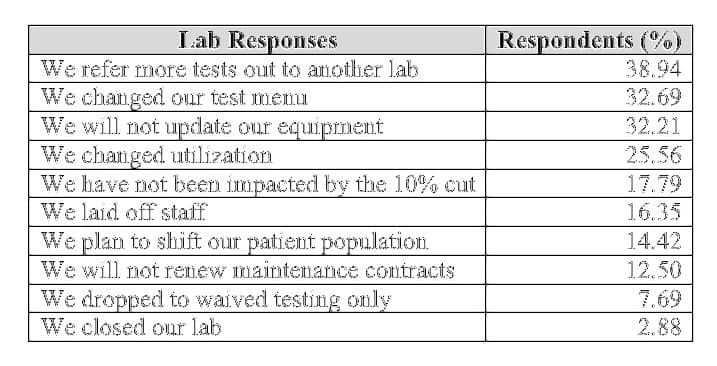
Table 1. Clinical laboratory responses to the first 10% cut in the Medicare clinical laboratory fee schedule (CLFS) resulting from implementation of the Protecting Access to Medicare Act of 2014 (PAMA), according to the “Clinical Laboratory Fee Schedule for Medicare” survey conducted by COLA, June–December, 2018.
Daly: What concerns us most is that the report did not include any discussion about how the PAMA-related cuts are affecting Medicare beneficiary access to near-patient testing. In our own data, we see early signals of future adverse effects on elderly access to laboratory services. For example, laying off staff, not updating equipment, and not renewing maintenance contracts strongly suggest the potential closing of the laboratory or further limitations on testing. Furthermore, nearly 39% of respondents to COLA’s surveys indicate that they are now “referring more tests out to another laboratory,” which can increase the timeframe for receiving test results needed for diagnosis, and create delays in initiating treatment. Our 2017 evaluative study revealed that near-patient testing performed in physician offices is for some communities the sole access to laboratory services, and without the immediacy of test results in the doctor’s office, patients would have died.
CLP: What kind of changes in GAO’s analysis will be most valuable as a corrective to its earlier report?
Daly: We must convey the value of near-patient testing as a vital part of any comprehensive national network of clinical laboratories. One respondent to our 2018 PAMA impact survey shared that, “Our patient described symptoms possibly indicating a heart attack and the patient was refusing to go to the emergency room, believing that he had heartburn. We performed a cardiac troponin in the office and immediately called 911. The patient had a cardiac cath within 2 hours of first arriving at our office.”
COLA has gathered hundreds of patient stories like this one. We shouldn’t overlook the unintended consequences of PAMA policies on elderly access to testing, the consequences of reduced access on early diagnosis and treatment, or the relationship of such policies to increased healthcare costs.
CLP: Is it likely that GAO’s recommendations would change as a result of an expanded report?
Daly: Since we have this data, we believe it is our responsibility to inform GAO that patients will be adversely affected. While I can’t predict the outcome, I can only hope that meaningful discussions about the effects of PAMA-related cuts on Medicare beneficiary access will be part of the discussions.
CLP: What other outcomes does COLA hope or expect to develop as a result of an expanded GAO report?
Daly: Every day, we visit laboratories across the country in a wide range of care settings, including ambulatory surgery centers, federally qualified health centers, health fairs, health maintenance organizations, healthcare systems, hospitals, independent laboratories, nursing facilities, physician offices, rural and community clinics, and student centers. Our hope is that the stories of how their patients are being affected by PAMA will be heard and taken seriously.
Steve Halasey is chief editor of CLP.
References
- Medicare Laboratory Tests: Implementation of New Rates May Lead to Billions in Excess Payments [GAO-19-67]. Washington, DC: Government Accountability Office, 2018. Available at: www.gao.gov/products/gao-19-67. Accessed February 26, 2019.
- COLA Requests Expansion of GAO Report on PAMA [press release, online]. Columbia, Md: COLA, 2019. Available at: www.cola.org/gao-report-pama-cuts. Accessed February 26, 2019.
- Taylor NP. Industry Strikes Back at GAO’s ‘Flawed and Dangerous’ PAMA Report [online]. Medtech Dive. Available at: www.medtechdive.com/news/industry-strikes-back-at-gaos-flawed-and-dangerous-pama-report/548331. Accessed February 27, 2019.



{kind=link}