Quantitative tissue-based diagnostics advance the promise of personalized medicine
By Ralf Huss, MD

Ralf Huss, MD, Definiens.
Immunotherapies—forms of treatment that leverage the body’s own immune system to help fight diseases—are increasingly being looked to as the future of cancer treatment.1 While such traditional methods of cancer treatment as radiation and chemotherapy focus primarily on targets associated with the patient’s tumor, immunotherapy enlists the body’s own internal defense system to combat cancer cell growth and metastasis.
Immunotherapy for cancer was first introduced in the late 1980s by Steven A. Rosenberg, MD, PhD, and several of his colleagues at the National Cancer Institute (NCI), when they published an article that reported a low tumor regression rate (2.6%–3.3%) among patients with metastatic cancer who underwent different types of active specific immunotherapy.2 Since then, a significant amount of research has been conducted on how to effectively activate the immune system to fight cancer. There are currently three main approaches to immunotherapy in oncology:
- Cancer vaccines. Substances that initiate a patient’s immune response against cancer cells, potentially used to prevent or treat cancer.3
- Immune checkpoint inhibitors. Drugs that prevent immune cells from being turned off (or checkpoints from working), enabling the immune system to continue doing its job of detecting and attacking cancer cells.3
- Advanced therapies, such as those making use of chimeric antigen receptor (CAR) T cells. CAR-T cell therapies use a technique known as adoptive cell transfer, by which T cells are collected from the patient and genetically engineered to express receptors specific to the particular form of cancer. The T cells can then recognize and kill the cancer cells, and are then reintroduced into the patient.4
A number of approved immunotherapies are currently on the market. Among the best known are Herceptin for HER2 breast cancer, and Keytruda and Yervoy for malignant melanoma.
With the early success of these and other immunotherapies, researchers have been encouraged to place greater emphasis on their work in this field. Consequently, there is currently a significant amount of immunotherapy research under way, and important results are being reported nearly every week. Results from a recent myeloma study, for example, showed that 70% of participants experienced a significant clinical response to immunotherapy.5 With the volume of immunotherapy research now being conducted, some analysts are predicting that immunotherapies will constitute 60% of all cancer treatments by 2024.6
NEW COMPLEXITIES
While immunotherapies hold promise, however, they also usher in new complexities. In particular, there is a need for better, faster ways to assess patient immune profiles in order to guide the application of immunotherapies. Consequently, the pharmaceutical and biotechnology companies involved in developing immunotherapies have also taken a strong interest in developing and leveraging companion diagnostics (CDx) that can help clinicians assess whether their patients may benefit from such therapies.
In order for immunotherapies to reach their true potential, CDx are needed.7 Such diagnostic tests provide important information about the safe and effective use of a corresponding drug or biological product. With the support of the clinical lab, they can help oncologists determine whether a particular drug’s benefits will outweigh any risks or potentially serious side effects to the patient.7
There are several types of organizations involved in developing CDx. Most major pharmaceutical companies are now either providing funding to diagnostics companies to develop them, or partnering with or acquiring diagnostics companies to improve their portfolios in the field. Earlier this year, for example, Roche, Basel, Switzerland, acquired a majority stake in Foundation Medicine, Cambridge, Mass, in order to advance its progress on personalized treatments for patients with cancer.8
While the primary developers of CDx are in vitro diagnostics manufacturers, clinical labs are increasingly getting involved in assay development, making use of their continuous access to clinical samples, which are needed for assay validation. To illustrate, Clarient, Aliso Viejo, Calif, was formerly primarily a service provider. However, the company has become increasingly involved in diagnostic test development, and was acquired in 2010 by GE Healthcare, Amersham, UK—and recently by NeoGenomics, Fort Myers, Fla—in part because of the company’s CDx development plans.9 While clinical labs currently play a minor role in assay development, and are predominately the end-users of such tests, they may eventually become more central to the process of CDx development.
This article will address several key issues related to the current state of diagnostic products and clinical laboratory testing for immunotherapies, including:
- The essential role of CDx—particularly tissue-based CDx—to guide the application of immunotherapy advances.
- Challenges and opportunities with regard to CDx development and unique considerations in harnessing contextual tissue information for diagnostics.
- Considerations for successful application of tissue-based CDx.
CDX IN IMMUNOTHERAPY
Immunotherapies hold a great deal of promise, but the current portfolio includes very few drugs that have received FDA approval to be marketed in the United States. Moreover, the commercially available drugs, most of which are checkpoint inhibitors, are so far approved for use only by patients who have already undergone and were unresponsive to the standard of care.
There is great potential for immunotherapy to be effectively used in early stages of treatment, when a patient’s immune system has not yet been affected by a chemotherapy or radiation regimen. However, in order to move immunotherapies into first- or second-line treatment, researchers and oncologists must first be able to identify the patients that would make appropriate candidates for the therapy. CDx help provide this information.
As mentioned earlier, CDx help determine the patients with the highest likelihood of responding to a therapy.10 Specifically, according to FDA, CDx provide information needed to: 10
- Identify patients who are most likely—or unlikely—to benefit from a particular therapy, and determine when and how often they should receive it.
- Identify patients likely to be at increased risk for serious side effects from the therapy.
- Monitor a patient’s response to therapy in order to adjust treatment as needed to achieve improved safety or effectiveness.
If the clinical lab does not have access to a diagnostic test that provides information to help reach the correct conclusion about a patient, a potentially responsive patient might not receive the therapy or, vice versa, a patient may undergo unnecessary and costly immunotherapy with little chance of benefit.11 In fact, a recent report by the Institute of Medicine noted significant issues with medical diagnoses in the United States, citing research that suggests diagnostic errors are implicated in one of every 10 patient deaths (not limited to cancer-related deaths).12
Having access to a robust CDx, on the other hand, enables the clinical lab to be a stronger partner in determining whether a patient is an acceptable candidate for therapy, and ultimately aids the oncologist and patient in making an informed decision about treatment. Leveraging CDx to guide the use of immunotherapy can improve patient outcomes and quality of life, as well as benefit payers and the healthcare system by improving care and reducing costs through the reduction of unnecessary treatments.
DIFFERING APPROACHES
As healthcare professionals look toward increased use of personalized medicine approaches to therapy, CDx will be vital to decisionmaking in immunotherapy.13 There are several approaches to cancer diagnostics that can be used in creating CDx—including immunoassays, amplification-based molecular assays, liquid biopsies, genetic testing, and tissue-based assays—each with its own unique strengths and weaknesses.
Immunoassays, such as those in the well-known enzyme-linked immunosorbent assay (ELISA) format, are chemical tests of a patient’s blood or other body fluids that detect or measure specific substances produced by the patient’s immunological response mechanisms.14 Immunoassays generally offer high sensitivity and specificity, and they make use of patient specimens that are readily available. However, the results of immunoassay testing can be significantly influenced by other diseases or infections a patient may have, so they are unreliable for developing robust cancer CDx.
Amplification-based molecular assays search for rare, tumor-specific mutations.15 Such tests usually require pathologists to know what they are looking for, since they can only amplify targets that are already known to be present. When using amplification-based tests, it may also be necessary to perform microdissecting procedures and to enrich for mutation-carrying cells, so that an understanding of the spatial relationships of any amplified signal with the morphology of the specimen can be maintained. But in the end, amplification-based assays have narrow sensitivity, making them unlikely candidates as the basis for CDx development.
There is currently a strong and growing interest in liquid biopsies—in particular, the analysis of DNA or RNA from a patient’s blood sample, which is easily accessible and can be continuously retrieved.16 Over the past decade, there has been a significant amount of research around circulating tumor cells (CTCs), resulting in an increasing number of important advances. Last year, for example, Bayer Pharma AG, Berlin, Germany, released findings from a study using the CellCollector by Gilupi GmbH, Potsdam, Germany, for the detection of CTCs in the blood, serving as a liquid biopsy and prognostic test for patients with castration-resistant prostate cancer.17 Nevertheless, liquid biopsies contain very little intelligence about where a cancer originated or how it is progressing. Consequently, no liquid-based assay has yet been proven useful in daily diagnostic routines, and it remains uncertain whether the method can be made convincing to the entire medical community.
Genetic testing is a viable option as the basis for CDx development. Since DNA testing and sequencing are standardized processes, this method of testing is fairly easy for labs to execute. However, genetic tests alone do not provide enough information about how the cancer is behaving in a certain patient, and thus whether the patient is a good candidate for a particular immunotherapy.
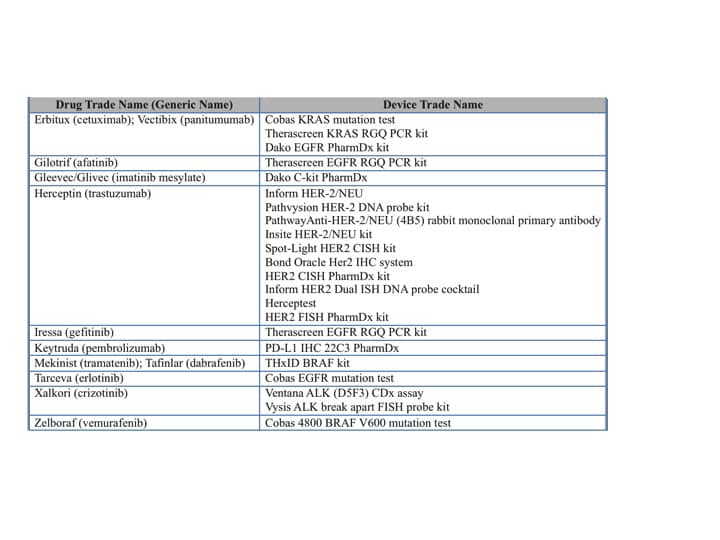
Table 1. FDA-approved tissue-based companion diagnostics. Click to enlarge.
For solid tumor cancers, the greatest CDx value lies with tissue-based approaches that position a patient’s tissue specimens at the center of diagnosis. In practice, oncologists do not initiate a course of treatment without a proper diagnosis, which is typically based on analysis of the patient’s tissue samples and how the cancer is behaving. Pathologists look to tissue analysis for information about where the cancer originated, how it is evolving, and how certain therapies are affecting the disease and its progression. Consequently, it makes sense that CDx and related treatment decisions should also be tissue-based. At present, however, there are very few tissue-based diagnostics available to support such treatment decisions (see Table 1).18
DEVELOPING TISSUE-BASED CDX
The number of tissue-based CDx known to be under development is rather meager, in part because developing them is a challenging endeavor, for several reasons.
Biomarker Identification. The biomarkers being identified and targeted for CDx are inducible. This means that if a patient has already undergone treatment, such as a regimen of chemotherapy, the expression of relevant biomarkers may be influenced and test results will be affected. Even the HER2 biomarker, one of the best-known and effective markers used in CDx, is not infallible. Research shows that the results of testing for HER2 status are incorrect in 8% of cases, and results can also vary depending on the area of the tumor being tested.19,20 Such findings suggest that there may be patients who test negative for the presence of the HER2 biomarker, and are thus technically not candidates for treatment, yet who will still respond to HER2 therapy.
In order to develop more robust tissue-based assays to identify the appropriate patients for immunotherapies, the markers used for CDx must be robust enough that they won’t be altered by external factors. Unfortunately, identifying them is often like searching for the proverbial needle in a haystack.
Lack of Robust Immunohistochemistry (IHC) Assays. IHC assays detect antigens or proteins in tissues and cells. They play an important role in drug development, where they are being used to test drug efficacy by detecting the activity of disease targets, and they are also being used in the development of tissue-based CDx. Although IHC is useful in many areas, the method is generally considered to be qualitative or semiquantitative, making it a challenging tool for identifying patient stratification lines and developing CDx.
The quality of tissue-based IHC assays can be influenced by a variety of factors, including the tissue collection and handling process—such as whether hospitals follow tissue collection protocols accurately—as well as antibody behavior. Also, there are many antibodies on the market that could be used in IHC assays, and it can be difficult for researchers to determine which is the most appropriate or will be sensitive enough for use in each case.21
Patient Stratification Cutpoints. One of the primary challenges with IHC is the relative weakness of the method for revealing cutpoints that represent meaningful differences for the purpose of patient stratification. When using IHC assays, in other words, pathologists can encounter difficulty identifying the points at which patients are categorized into potential responders or nonresponders for a particular therapy.
With traditional IHC assays, the pathologist stains the tissue and then selects a cutpoint based on visual inspection of the distinctive expression levels identified by the antibody. If the antibody performs well and binds to a highly expressed protein, that’s where the cutpoint will be drawn, or “binned,” since the pathologist uses the bound stain to see and grade the expression level in the specimen (eg, 1+, 2+, or 3+). Even when it is successful, this method of assigning cutpoints can be somewhat imprecise, since it is based on the antibody’s behavior in relation to a specified metric or variable with biological relevance. Worse still, if the antibody does not select for expression levels that are significant mechanistically or from a biological standpoint, the pathologist could miss entire expression levels important to stratifying the patient. Ultimately, if a reliable and meaningful cutpoint can’t be found, the assay can’t be used to stratify patients and determine who is a match for a particular therapy.
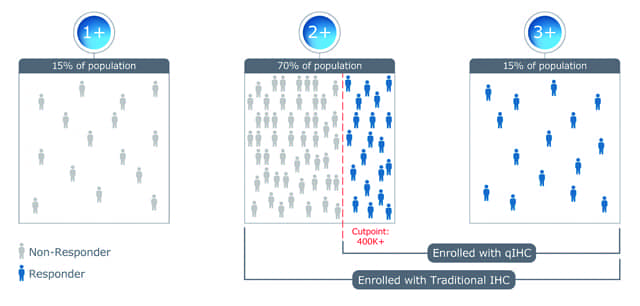
Figure 1. Traditional immunohistochemistry methods often enroll a large number of nonresponders in a clinical trial.
In a common clinical trial scenario, traditional IHC methods show patients in the 2+ and 3+ population to be potential drug responders, with the 2+ population making up 70% of the patients, and they are thus all enrolled in the trial (see Figure 1). However, the majority of the 2+ population are actually nonresponders, with the result being that the trial fails to demonstrate the medical value of the drug. In turn, failure of the trial ultimately results in either no further development of the drug, or 20% of the population not receiving a valuable treatment.
LEVERAGING CONTEXTUAL TISSUE CLUES
Despite such challenges, there are opportunities for advances growing from the use of tissue-based CDx. Although IHC assays are not currently being used in an absolutely quantitative way, they can be made more standardized and quantitative in order to effectively identify patient stratification thresholds and provide robust CDx. Doing so will require digitization of images and the use of image analysis, and for IHC pathology to become a quantitative rather than a descriptive discipline.22
In terms of biomarker identification, a primary obstacle for researchers is the inability to visualize the spatial distribution of immune cells and their correlation to the tumor—information that is needed in order to effectively identify robust biomarkers. However, it is possible to visualize the spatial relationships of immune cells within a tumor through the use of powerful tissue image analysis tools, a practice that is becoming increasingly common across research labs.
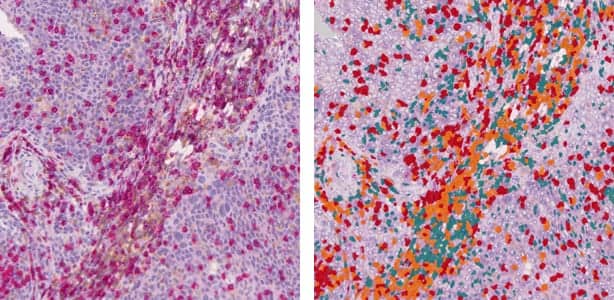
Figure 2. On the left, a traditional digital tissue slide. On the right, automated image analysis enables contextual measurement of immune response in the tumor microenvironment through the detection, classification, and quantification of lymphocytes (stained with CD3 and CD8).
Using image analysis tools to review digitized tissue slides, pathologists can collect all the useful and relevant data from a tissue sample and view it in context, while also seeing important spatial relationships. By leveraging the contextual information contained in such digitized tissue, pathologists can identify cutpoints based on measured features or other biologically relevant variables that can’t be seen by visual observation or understood by antibody behavior alone (see Figure 2).
The application of such detailed tissue-based image analysis to the development of CDx has the potential to significantly alter the outcome of a clinical trial scenario similar to that described above (see Figure 3). Where a traditional IHC assay might not be sensitive enough to identify the biologically relevant cutpoint between responders and nonresponders for the proposed immunotherapy, a quantitative IHC (qIHC) approach can enable researchers to identify the appropriate cutpoint (in this example, at 25,000 proteins/cell) and to enroll the correct patient population in the trial.
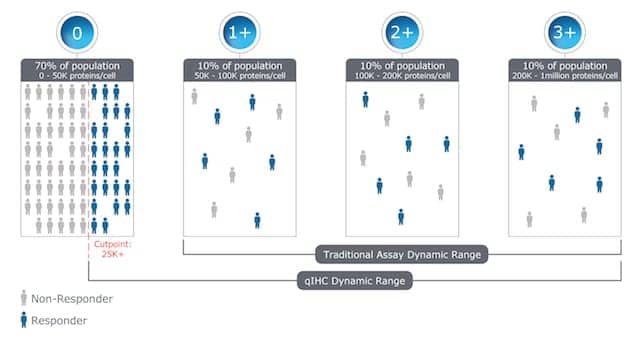
Figure 3. Using quantitative immunohistochemistry methods, pathologists can find the cutpoint or patient stratification line, and thus better identify patients most likely to respond to a particular therapy.
Researchers are working to generate the data needed to support the development and adoption of CDx and prognostic tests for immunotherapy using such tissue-based image analysis methods. The Immunoscore Project—a global task force led by the Society for Immunotherapy of Cancer—has taken on the task of validating and promoting the inclusion of immunological biomarkers in the prediction of a patient’s prognosis and response to therapy. The group’s new approach, termed the “immunoscore,” rests on an evaluation of the patient’s immunological biomarkers and immune response to a tumor, rather than on classification and staging of the tumor itself. 23 The immunoscore concept is currently being validated in 17 countries, and results are expected in 2016.24 Should results be positive, the project may spur additional industry interest—primarily among pharmaceutical and diagnostics companies—in leveraging image analysis and qIHC for the development of CDx.
SUCCESSFUL CDX APPLICATION IN THE LAB
Developing CDx and moving them into the marketplace for everyday clinical use will no doubt take time, part of which will need to be devoted to meeting the stringent regulatory requirements related to the development of CDx.
In the United States, FDA requires an investigational device exemption (IDE) for any assay being used for patient stratification during investigative trials. Unless they are exempt, all clinical evaluations of investigational devices must have an approved IDE before the study is initiated.25 Clinical studies can then be conducted to support the sponsor’s premarket approval (PMA) application, through which FDA conducts a rigorous scientific and regulatory review to evaluate the safety and effectiveness of medical devices.
The European Union and other regions and countries that recognize CE marking do not require an IDE or equivalent to use a patient stratification assay during the investigative phase. However, a CE mark is required to commercialize and distribute any assay used for patient stratification to determine the therapy a patient may receive.26
The PMA and CE mark designations are required to demonstrate that diagnostics developers are in compliance with all manufacturing and clinical regulations. But once a tissue-based CDx has actually been approved for use commercially, a new set of challenges arises.
In a typical scenario, when a new CDx-guided drug is developed, the pharma company will make doctors aware that the drug may benefit patients who express a certain biomarker within a specified range. To determine if a particular patient is a match for the drug, the oncologist sends a tissue sample to the lab, asking if the patient falls into the specified range of responders. At this point, it is up to the lab to make a definitive conclusion about the status of the patient. But even when a lab is running an approved test with an assigned antibody—meaning that the procedure, methods, and readouts are “locked” and cannot change—there may still be uncertainties.
With tissue-based assays, a lab’s ability to determine whether a patient may be a responder resides in several factors. First, the lab must rely on tissue samples from sources over which they usually have no control. In order for the assay to work as planned, the tissue images must be of sufficient quality and contain the information needed for proper analysis. At present, however, tissue gathering and handling protocols are not standardized across countries or even across labs, and different sites may handle their tissue samples differently. Such preanalytical inconsistencies can lead to very different test results.
Second, the test readouts are subject to interpretation. Whereas the results of clinical chemistry assays provide an absolute value that is not open to interpretation, tissue-based assays such as HercepTest provide semiquantitative scores that must be interpreted by the pathologist.27 Diagnostics developers are working toward creating test readouts that are more quantifiable—for example, assigning meaning to such measurements as the number of cells in a certain area—but until such standard metrics have become accepted in everyday practice, it will no doubt remain challenging for labs to interpret tissue-based test results.
On the other hand, clinical lab personnel can play a role in the improvement of CDx by sharing patient response data they are gathering. Such information can be used to measure and compare changes in the assay over time, so that pharmaceutical and diagnostics companies can make more-informed decisions, and potential adjustments, based on a drug’s performance within specific patient populations.
The National Institutes of Health (NIH) has developed data sharing repositories that make a variety of data accessible for reuse by other labs and organizations—including cancer medical images, analysis tools, and assay results.28 Organizations such as NCI and various universities and research institutions manage the individual repositories, and most accept submissions of data from NIH-funded investigators as well as others working in the field.28 The data contained in the repositories are open for use by the entire research and medical community. The Cancer Nanotechnology Laboratory repository by NCI, for example, is designed to facilitate information-sharing across the international biomedical nanotechnology research community, and to expedite and validate the use of nanotechnology in biomedicine.29 The repositories also include resources that aggregate information about biomedical data and information-sharing systems.
Data mining and cross-lab data-sharing, such as through the NIH repositories, will be important for the success of CDx in immunotherapy. Such activities will enable clinical lab professionals to make decisions based on larger datasets, rather than coming to conclusions based on a narrow view of drug response data from their own individual labs.
CONCLUSION
The existence of more-robust CDx is essential for the advancement of the immunotherapy field. Since solid tumor cancer diagnoses come from the tissue, effective CDx for immunotherapy will likely be tissue-based. In the coming years, many more clinical validation trials on tissue-based CDx are expected, since a test’s reliability can only be proven in larger and well-designed clinical trials.
While there are challenges for the development of tissue-based CDx, creating more quantifiable assays will help enhance patient stratification and lead to more-robust CDx for use by clinical labs. Such tests will ultimately enable lab professionals to provide stronger test results, allow oncologists to make more confident treatment decisions, and help to advance personalized medicine.
Ralf Huss, MD, is chief medical officer at Definiens. For further information, contact CLP chief editor Steve Halasey via [email protected].
REFERENCES
- Couzin-Frankel J. Breakthrough of the year 2013: cancer immunotherapy. Science. 2013;342(6165):1432–1433; doi: 10.1126/science.342.6165.1432.
- Rosenberg SA. Adoptive immunotherapy of cancer: accomplishments and prospects. Cancer Treat Rep. 1984;68(1):233–255.
- Types of cancer immunotherapy [online]. Atlanta: American Cancer Society, 2015. Available at: www.cancer.org/treatment/treatmentsandsideeffects/treatmenttypes/immunotherapy/immunotherapy-what-is-immunotherapy. Accessed October 21, 2015.
- Rapoport AP, Stadtmauer EA, Binder-Scholl GK, et al. NY-ESO-1–specific TCR-engineered T cells mediate sustained antigen-specific antitumor effects in myeloma. Nat Med. 2015;21(8): 914–921; doi: 10.1038/nm.3910.
- Ledford H. Cancer treatment: the killer within. Nature. 2014;508(7494):24–26; doi: 10.1038/508024a.
- In vitro companion diagnostics: guidance for industry and Food and Drug Administration staff. Silver Spring, Md: Food and Drug Administration, 2014. Available at: www.fda.gov/downloads/MedicalDevices/DeviceRegulationandGuidance/GuidanceDocuments/UCM262327.pdf. Accessed October 21, 2015.
- Roche enters a broad strategic collaboration with Foundation Medicine in the field of molecular information in oncology [press release]. Basel, Switzerland: Roche, 2015. Available at: www.roche.com/media/store/releases/med-cor-2015-01-12.htm. Accessed October 26, 2015.
- FDA takes steps to help ensure the reliability of certain diagnostic tests [press release]. Silver Spring, Md: Food and Drug Administration, 2014. Available at: www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm407321.htm. Accessed October 21, 2015.
- National Academies of Sciences, Engineering, and Medicine. Improving diagnosis in healthcare. Balogh EP, Miller BT, Ball JR, eds. Washington, DC: The National Academies Press, 2015.
- Personalized medicine and companion diagnostics go hand-in-hand [online]. Silver Spring, Md: Food and Drug Administration, 2014. Available at: www.fda.gov/ForConsumers/ConsumerUpdates/ucm407328.htm. Accessed October 21, 2015.
- What is an immunoassay? [online]. Bloomington, Minn: ImmunoChemistry Technologies, 2010. Available at: www.immunochemistry.com/resource/what-immunoassay. Accessed October 27, 2015.
- Types of molecular tumor testing [online]. Nashville, Tenn: My Cancer Genome, 2015. www.mycancergenome.org/content/molecular-medicine/types-of-molecular-tumor-testing/. Accessed October 27, 2015.
- Gallagher J. Blood test ‘boost’ in ovarian cancer fight. BBC. May 5, 2015. Available at: www.bbc.com/news/health-32530339. Accessed October 21, 2015.
- Theil G, Haubold K, Fornara P, et al. Comparison of CTC capture efficiency of the CellCollector technology versus CellSearch in prostate cancer patients at multiple time points [presentation abstract]. Cancer Res. 2014;74(19 suppl):abstract no 3474; doi: 10.1158/1538-7445.AM2014-3474.
- HER2 status [online]. Ardmore, Penn: BreastCancer.org, 2015. Available at: www.breastcancer.org/symptoms/diagnosis/her2. Accessed October 21, 2015.
- Luongo de Matos L, Trufelli DC, Luongo de Matos MG, Aparecida da Silva Pinhal M. Immunohistochemistry as an important tool in biomarkers detection and clinical practice. Biomark Insights. 2010; 5:9–20. doi:10.4137/BMI.S2185.
- Dunstan RW, Wharton KA, Quigley C, Lowe A. The use of immunohistochemistry for biomarker assessment—can it compete with other technologies? Toxicology Pathol. 2011;39(6): 988–1002; doi: 10.1177/0192623311419163.
- Immunoscore project. Milwaukee: Society for Immunotherapy of Cancer, 2015. Available at: www.sitcancer.org/about-sitc/initiatives/immunoscore. Accessed October 21, 2015.
- Galon J, Pages F, Marincola FM, et al. Cancer classification using the immunoscore: a worldwide task force. J Transl Med. 2012;10:205; doi: 10.1186/1479-5876-10-205.
- NIH data sharing repositories. Bethesda, Md: NIH National Library of Medicine, 2015. Available at: www.nlm.nih.gov/NIHbmic/nih_data_sharing_repositories.html. Accessed October 21, 2015.
- caNanoLab FAQ. Bethesda, Md: National Cancer Institute, 2015. Available at: https://wiki.nci.nih.gov/display/caNanoLab/caNanoLab+FAQ#caNanoLabFAQ-HowdoIsubmitdataintocaNanoLab. Accessed October 27, 2015.
- CAR T-cell therapy: engineering patients’ immune cells to treat their cancers [online]. Bethesda: National Cancer Institute, 2015. Available at: www.cancer.gov/about-cancer/treatment/research/car-t-cells. Accessed October 26, 2015.
- Stynes T. NeoGenomics to acquire GE cancer testing unit Clarient. Wall Street Journal. October 21, 2015. Available at: www.wsj.com/articles/neogenomics-to-acquire-ge-cancer-testing-unit-clarient-1445431725. Accessed October 27, 2015.
- Companion diagnostics [online]. Silver Spring, Md: Center for Devices and Radiological Health, FDA, 2014. Available at: www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/InVitroDiagnostics/ucm407297.htm. Accessed October 21, 2015.
- List of cleared or approved companion diagnostic devices (in vitro and imaging tools) [online]. Silver Spring, Md: Food and Drug Administration, 2015.Available at: www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/InVitroDiagnostics/ucm301431.htm. Accessed October 21, 2015.
- Consider second opinion if HER2 test is negative. Ardmore, Penn: BreastCancer.org, 2010. Available at: http://www.breastcancer.org/research-news/20101214. Accessed October 21, 2015.
- Device advice: investigational device exemption (IDE) [online]. Silver Spring, MD: Food and Drug Administration, 2015. Available at: www.fda.gov/MedicalDevices/DeviceRegulationandGuidance/HowtoMarketYourDevice/InvestigationalDeviceExemptionIDE/. Accessed October 27, 2015.
- CE marking. London: UK Government, 2012. Available at: www.gov.uk/guidance/ce-marking. Accessed October 27, 2015.
- HercepTest. Carpinteria, Calif: Dako, 2015. Available at: www.dako.com/us/ar39/p101510/prod_products.htm. Accessed October 27, 2015.



{kind=link}