Emerging ultrasensitive tests promise a paradigm shift in immunodiagnostics
By John Todd, PhD
Over the past half-century, immunoassays have become important tools in both research and clinical laboratories. An ongoing challenge for such immunoassay technologies has always been their relative lack of the sensitivity needed for accurate diagnosis and rule-out of disease. With single molecule counting technologies now making possible ultrasensitive immunoassays, however, a paradigm shift is under way for the field of immunodiagnostics.
Discovery and Development
The first immunoassay was developed in the 1950s by Solomon Berson, MD, and Rosalyn Yalow, PhD, of the Bronx Veterans Administration Medical Center.1,2 The immunoassay they created was a radioimmunoassay using radioactive iodine-131. It was initially developed for use in measuring the concentration of insulin in plasma specimens, and was subsequently modified for the measurement of other hormones. In 1977, Yalow received the Nobel Prize in Physiology or Medicine for this work.

John Todd, PhD, Singulex.
During the following decades, the immunoassay technology was further developed and refined, and announcements of multiple new radioimmunoassays were published. In time, the use of radioisotopes was replaced by the use of enzymes, leading to the development of the enzyme immunoassay (EIA) and enzyme-linked immunosorbent assay (ELISA) technologies.3,4 The discovery of the enzyme-multiplied immunoassay technique (EMIT) and other homogeneous immunoassays simplified the technology and allowed for automation.5 The application of chemiluminescent labels further improved analytical sensitivity.6
While early immunoassays relied upon antibodies purified from animals, the development of techniques for producing monoclonal antibodies from cell cultures enabled the manufacturing of larger quantities, and was awarded the Nobel Prize in Physiology or Medicine in 1984.7 In turn, this achievement allowed for the development of noncompetitive sandwich immunoassays, an approach that enhanced analytical sensitivity but required larger quantities of antibodies.
Today, immunoassay platforms capable of automatized analysis allow for high-throughput testing and are a mainstay in clinical laboratories. In addition, the development of lateral-flow tests has brought the technology from healthcare facilities to decentralized settings.
Although a mainstay of clinical diagnostic laboratories, the utility of such automated immunoassays has been limited by their relatively poor sensitivity and precision at low concentrations of analytes. The limits of sensitivity have been mainly the result of high background noise blocking the measurement of analyte signals at low concentrations. Thus, the holy grail of immunoassay development has been to enhance analyte signal while decreasing the background noise, commonly measured as the signal-to-noise (S/N) ratio.
Dawn of Ultrasensitive Immunoassays
The recent development of high-sensitivity immunoassays ushers in a new era for immunodiagnostics. Single molecule counting or detection technology, linked with traditional immunoassay technology, has made it possible to realize the holy grail of immunoassay development—specifically, improving the signal-to-noise ratio of an assay by up to a thousand-fold.
When polymerase chain reaction (PCR) technology was introduced to clinical laboratories, it led to significant improvements in the analytical sensitivity of molecular diagnostics. However, PCR-based tests can be hampered by high costs and poor precision. The evolution of high-sensitivity immunoassays has enabled detection of low-abundance molecules, approaching the clinical sensitivity accomplished with PCR.
Newly developed capabilities for detecting and quantifying biomarkers at low concentrations are changing clinical practice and patient management. Biomarker measurement has many applications, including risk stratification, disease detection, staging, prognosis determination, and monitoring. With a wide range of diagnostic opportunities, high-sensitivity immunoassays have the potential for a great and growing clinical impact.
The ability to rule-out disease is critical for an accurate, safe, and cost-effective diagnostic workup. High-sensitivity immunoassays may allow for such a paradigm shift, not only in detecting and diagnosing disease, but also in ruling-out disease, thereby eliminating unnecessary testing, and ultimately improving patient care.

Figure 1. The Sgx Clarity by Singulex, a fully automated in vitro diagnostic platform employing single molecule counting technology to detect analytes down to femtogram-per-milliliter levels.
A proprietary single molecule counting technology by Singulex, Alameda, Calif, aims to take immunodiagnostics to the next level by offering sensitivity up to a thousand times greater than contemporary immunoassay platforms. The company’s ultrasensitive, fully automated, quantitative, fluorescent, sandwich immunoassay allows for detection of analytes down to femtogram-per-milliliter levels. The single molecule counting digital detection technology has been developed for a fully automated in vitro diagnostic platform, the Sgx Clarity system (see Figure 1).
Singulex was founded in 2004, with the mission of bringing ultrasensitive immunodiagnostics to scientists and clinicians. In 2015, Singulex’s Erenna system, a research use only (RUO) platform, was acquired by EMD Millipore, the life science research business of Merck KGaA. In 2016, Grifols acquired a license to Singulex’s single molecule counting technology for pathogen detection in blood-screening applications. Today, Singulex is developing a broad analyte menu for the Sgx Clarity system, which is expected to be available in the European Union following CE marking of the instrument earlier this year. Singulex further plans to launch the Clarity system in the United States, subsequent to FDA clearance.
Single Molecule Counting
The Sgx Clarity system is based on a microparticle immunoassay powered by single molecule counting technology. During the capture step, microparticles are coated with specific antibodies. The surface chemistry of the microparticles improves binding efficiency while minimizing nonspecific binding. After capture, the microparticles are magnetically separated and washed to remove unbound proteins and any remnants of nonspecific binding.

Figure 2. Ultrasensitive single molecule counting technology used in the Sgx Clarity system from Singulex. A bright dye and optimized confocal optic system increase the signal, and low nonspecific binding and a very small interrogation space minimize background fluorescence.
Specific fluorescent dye-labeled detection antibodies translate each captured analyte into a signal. After isolation, each signal corresponds to a single analyte molecule. Elution volume is reduced to concentrate the signal and enhance the single molecule counting process. The eluate is then transferred to a microwell plate and loaded into the fully automated Sgx Clarity instrument for reading.
Single molecule counting is performed directly inside individual plate wells. Inside the well, a very small interrogation space is illuminated by a laser, which scans along a helical path, ensuring efficient signal capture. Single fluorescent-labeled molecules generate intense flashes of light as they are scanned (see Figure 2).
During counting, the intensity of the fluorescence encountered in the interrogation space is captured as a function of time. The measured fluorescence is sequestered in 100 microsecond time bins. Detected signals with peak intensity above the threshold of background fluorescence are counted as digital events, and the instrument records the sum of all digital events counted. At high concentrations, a proprietary algorithm computes the sum of all photons recorded; thus, a dynamic range of over six logs is achieved. Singulex’s single molecule counting technology allows for ultrasensitivity and broader dynamic range than contemporary assays.8
First Application: Cardiac Troponin
Now commercially available in the European Union, and available as an RUO instrument in the United States, Singulex’s single molecule counting technology has been validated in more than 130 peer-reviewed publications—predominantly, but not exclusively, for cardiovascular applications. The use of such a precise tool for early detection and rule-out of coronary artery disease (CAD) and acute myocardial infarction (AMI) may avoid unnecessary diagnostic testing, reduce healthcare costs, and improve patient care.
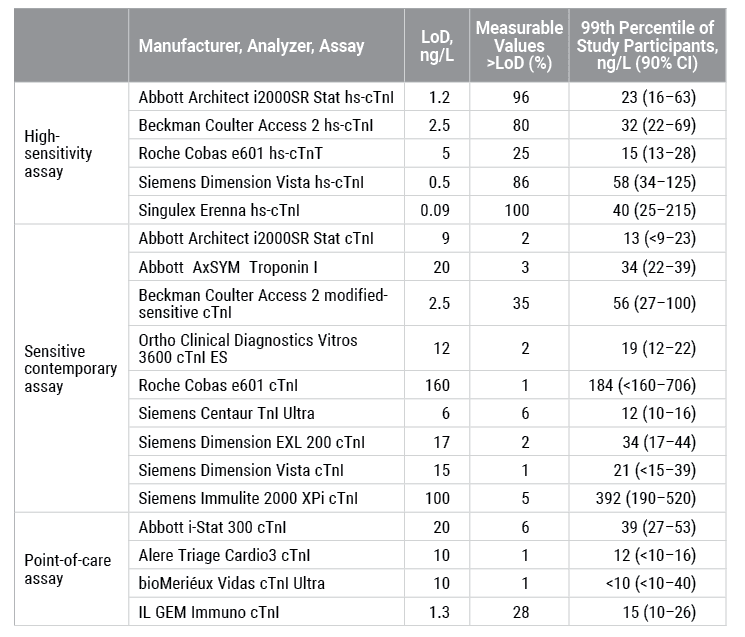
Table 1. Lower limit of detection (LoD) and 99th percentile values in a presumably healthy population measured by high-sensitivity, sensitive-contemporary, and point-of-care cTnI and cTnT assays, including Singulex’s cTnI assay for research use only (reproduced by permission of the American Association for Clinical Chemistry).15
Cardiac troponins I (cTnI) and T (cTnT) are used in the management of suspected AMI and have been associated with risk of future cardiovascular disease (CVD).9–11 But until recently, available assays have not been sufficiently sensitive to detect cTnI among healthy people. Singulex was the first research group to measure cTnI, a marker with low biological variability, in 100% of a group of presumably healthy individuals.12–14 When comparing the lower limit of detection and measurable values greater than the limit of detection among 19 cTnI and cTnT assays, the RUO single molecule counting assay from Singulex showed superior performance compared to contemporary cTnI assays (see Table 1).15
Plasma- or serum-based cardiac troponin tests have been shown to be capable of differentiating healthy patients from those that either have CVD or are at risk for developing CVD. In individuals without known risks for CVD, cTnI assays using single molecule counting technologies have been shown to predict risk of cardiovascular death, incident congestive heart failure (CHF), major adverse cardiovascular events, and all-cause mortality.9–11
In a comparison of Singulex’s single molecule counting RUO cTnI assay with two commercially available cTnI assays (Stat troponin I immunoassay and Architect Stat highly sensitive troponin I immunoassay; both performed on the Architect i2000SR immunoassay analyzer by Abbott Diagnostics, Abbott Park, Ill), the Singulex ultrasensitive assay had a stronger association with cardiovascular outcomes.10

Figure 3. The ultrasensitive cardiac troponin I assay by Singulex is CE marked and developed for use on the Sgx Clarity system.
In patients with stable CAD and recent acute coronary syndrome (ACS), monitoring of single molecule counting cTnI was shown to predict cardiovascular death and CHF. Such results can be used to guide therapy: patients with high cTnI levels 30 days after ACS had a reduction in cardiovascular death and CHF with high-intensity compared with moderate-intensity statin therapy.16 It has been further demonstrated that cTnI is predictive of CAD and is reduced by statin therapy.17
Measurement of cTnI is standard in the management of patients with suspected AMI.18 When evaluating presentation cTnI values in order to rule-in or rule-out AMI, the Singulex RUO cTnI single molecule counting assay has excellent sensitivity and negative predictive value when compared to a contemporary commercially available assay (TnI-Ultra; Siemens Healthineers, Tarrytown, NY).19 The ability to rule-in and rule-out AMI and non-ST-segment elevation myocardial infarction (NSTEMI) has been further demonstrated using the Singulex RUO cTnI assay for evaluating cTnI at presentation and for evaluating postpresentation changes in cTnI levels.20,21
Singulex has developed and CE marked a cTnI assay for use on the Sgx Clarity system (see Figure 3). Testing of that assay’s analytical performance characteristics shows that the limits of blank (LoB) and limits of detection (LoD) are 0.02 and 0.08 pg/mL, respectively. The assay’s limit of quantification (LoQ) is estimated to be 0.14 pg/mL at 20% CV, and 0.53 pg/mL at 10% CV, with observed precision in the range from 4.0% to 9.6%. The 99th percentile is 8.67 pg/mL (95% CI, 6.68–29.16).22
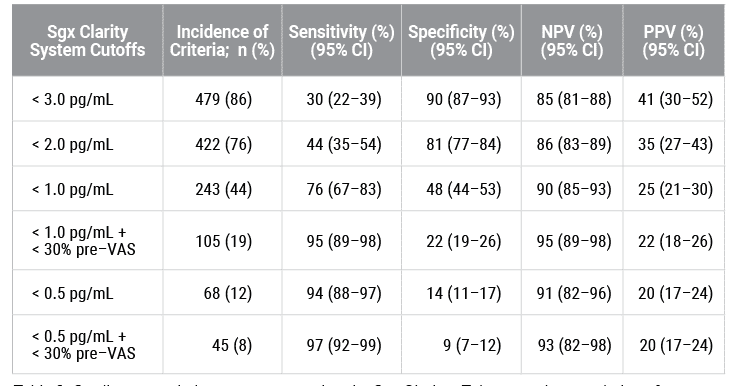
Table 2. Cardiac troponin I measurement using the Sgx Clarity cTnI assay: characteristics of prespecified cutoff values.22
To reduce the public health burden of CAD, early detection of the disease is critical. Cardiac stress testing is the mainstay of noninvasive CAD diagnostics. Nuclear stress testing with imaging, such as myocardial perfusion imaging single-photon emission computed tomography (MPI-SPECT), has limitations, including a poor diagnostic yield, high costs, limited availability, and exposure to contrast agents and radiation.23 Consequently, there is a need for developing more cost-effective strategies for the initial work-up of patients who are presently at low risk of manifesting inducible myocardial ischemia during cardiac imaging procedures. In addition to reducing healthcare costs, an alternative rule-out tool would reduce patient time in medical facilities and the number of specialist referrals needed. In a study of 555 patients without previously known CAD referred for stress MPI-SPECT imaging, cTnI measurements using the Sgx Clarity cTnI assay were obtained before stress testing. When cTnI test results were <0.50 pg/mL, the test had a sensitivity of 94% and negative predictive value (NPV) of 91% for ruling-out cardiac ischemia. Combining clinical judgment using visual analog scale (VAS) assessment with a cTnI prestress test increased the ability to rule-out the presence of cardiac ischemia at an NPV of 93% (see Table 2).22 In addition, the single molecule counting RUO cTnI assay has been shown to be predictive of obstructive CAD.24
Advancing Clinical Research
Singulex is expanding clinical evaluation of the Sgx Clarity system at a number of research sites in the European Union. In collaboration with Jordi Ordóñez-Llanos, MD, PhD, professor of clinical biochemistry at Hospital de la Santa Creu i Sant Pau, Barcelona, clinical research studies evaluating the value of single molecule counting technology for cTnI assessment in patients suspected of having ACS, including AMI, are currently underway.
According to Ordóñez-Llanos, “Singulex’s proprietary single molecule counting technology is already proven to have improved cTnI detection and clinical sensitivity, thus increasing the performance of the biomarker to evaluate ACS and, particularly, AMI.
“With that clinically proven power now available in an in vitro diagnostics platform, researchers like me can have direct access and explore the potential for clinical use,” he adds. “At my site in Barcelona, we’ve already demonstrated precision and functional sensitivity and are expanding clinical research studies to explore applications of the cTnI to better understand heart disease status.”
At St. George’s University, London, Paul O. Collinson, MBBChir, MD, FRCPath, FACB, FRCP, professor of cardiovascular biomarkers, has completed analytical evaluation of the Sgx Clarity system’s performance. Collinson will go on to test the Westcor study to investigate the ability of hs-cTnI assays to rule out the presence of AMI.
“We have observed performance of the Sgx Clarity cTnl assay at the level which we believe meets the European Society of Cardiology guidelines for the management of acute coronary syndromes, specifically to rule-in and rule-out patients,” says Collinson. “In our view, this validates the utility of Singulex’s in vitro diagnostics platform and reinforces the opportunity it may present to our understanding of heart and total health status.”
Anthony Freemont, MD, FRCP, FRCPath, director of the molecular pathology innovation center at the University of Manchester, and Richard Body, MBChB, PhD, MRCSEd(A&E), FCEM, professor of the Royal College of Emergency Medicine, are testing the Sgx Clarity cTnI assay in the supersensitive troponin admission reduction (STAR) study. The study is an evaluation of patients across the UK with cardiac chest pain to determine whether use of the ultrasensitive Sgx Clarity cTnI assay can rule-out ACS, lead to lower readmission rates, and bring cost savings to the UK’s National Health Service.
Future Directions
In April of this year, the Sgx Clarity system achieved the CE mark, making it eligible for marketing in Europe and other countries that accept the mark. Singulex plans to submit the system for FDA premarket notification (510(k)) clearance during the second half of this year.
To expand the future Sgx Clarity test menu beyond cTnI, Singulex is currently developing additional assays, including assays for procalcitonin and Clostridium difficile toxins A and B. Procalcitonin has been shown to aid in the diagnosis of severe sepsis.25 Testing for procalcitonin on the Sgx Clarity system may allow for rule-out of sepsis and subsequently guide antibiotic stewardship.
Diagnosis of C. difficile infection is challenging, in part because the currently available arsenal is dominated by immunoassays with relatively low sensitivity and molecular tests with low clinical specificity. It is intended that the Sgx Clarity C. difficile assay will achieve improved accuracy, making it a critical diagnostic tool for patients with suspected C. difficile infection.
Singulex is also in the process of developing a point-of-care instrument. The company’s goal is to have a prototype device ready by the end of 2017. It is expected that such a point-of-care system will facilitate patient-centered care, allow for more rapid turnaround times and immediate decisionmaking, and result in less fragmented healthcare.
In an effort to enter strategic collaborations, Singulex has recently partnered with Qiagen, Germantown, Md, to codevelop companion diagnostics. Singulex will contribute immunoassay capacity to Qiagen’s molecular testing services, when offering companion diagnostic capabilities to the pharmaceutical industry.
Conclusion
The evolution from Berson and Yalow’s first radioimmunoassay to today’s ultrasensitive single molecule counting technology spans nearly 6 decades. Immunoassays fundamentally changed clinical practice, and with the advancement of ultrasensitive immunoassays, the next disruption in healthcare will follow.
The Sgx Clarity system offers ultrasensitive biomarker detection that has the potential to support a paradigm shift in patient management. With unprecedented sensitivity, the single molecule counting technology will transform immunodiagnostics across multiple disease areas in both acute and chronic disease management, and change patient care from reactive disease treatment to proactive health management.
John Todd, PhD, is chief scientific officer at Singulex. For further information contact CLP chief editor Steve Halasey via [email protected].
References
- Yalow RS, Berson SA. Assay of plasma insulin in human subjects by immunological methods. Nature. 1959;184 (Suppl 21):1648–1649.
- Wu AHB. A selected history and future of immunoassay development and applications in clinical chemistry. Clin Chim Acta Int J Clin Chem. 2006;369(2):119–124; doi: 10.1016/j.cca.2006.02.045.
- Van Weemen BK, Schuurs AHWM. Immunoassay using antigen-enzyme conjugates. FEBS Lett. 1971;15(3):232–236.
- Engvall E, Perlmann P. Enzyme-linked immunosorbent assay (ELISA): quantitative assay of immunoglobulin G. Immunochemistry. 1971;8(9):871–874.
- Rubenstein KE, Schneider RS, Ullman EF. “Homogeneous” enzyme immunoassay: a new immunochemical technique. Biochem Biophys Res Commun. 1972;47(4):846–851.
- Schroeder HR, Vogelhut PO, Carrico RJ, Boguslaski RC, Buckler RT. Competitive protein binding assay for biotin monitored by chemiluminescence. Anal Chem. 1976;48(13):1933–1937.
- Köhler G, Milstein C. Continuous cultures of fused cells secreting antibody of predefined specificity. Nature. 1975;256(5517):495–497.
- Todd J, Freese B, Lu A, et al. Ultrasensitive flow-based immunoassays using single-molecule counting. Clin Chem. 2007;53(11):1990–1995; doi: 10.1373/clinchem.2007.091181.
- Wang TJ, Wollert KC, Larson MG, et al. Prognostic utility of novel biomarkers of cardiovascular stress: the Framingham Heart Study. Circulation. 2012;126(13):1596–1604; doi: 10.1161/circulationaha.112.129437.
- Neumann JT, Havulinna AS, Zeller T, et al. Comparison of three troponins as predictors of future cardiovascular events: prospective results from the FINRISK and BiomaCaRE studies. PloS One. 2014;9(3):e90063; doi: 10.1371/journal.pone.0090063.
- Apple FS, Steffen LM, Pearce LA, Murakami MM, Luepker RV. Increased cardiac troponin I as measured by a high-sensitivity assay is associated with high odds of cardiovascular death: the Minnesota Heart Survey. Clin Chem. 2012;58(5):930–935; doi: 10.1373/clinchem.2011.179176.
- Wu AHB, Lu QA, Todd J, Moecks J, Wians F. Short- and long-term biological variation in cardiac troponin I measured with a high-sensitivity assay: implications for clinical practice. Clin Chem. 2009;55(1):52–58; doi: 10.1373/clinchem.2008.107391.
- Wu AHB, Akhigbe P, Wians F. Long-term biological variation in cardiac troponin I. Clin Biochem. 2012;45(10–11):714–716; doi: 10.1016/j.clinbiochem.2012.03.008.
- Apple FS, Simpson PA, Murakami MM. Defining the serum 99th percentile in a normal reference population measured by a high-sensitivity cardiac troponin I assay. Clin Biochem. 2010;43(12):1034–1036; doi: 10.1016/j.clinbiochem.2010.05.014.
- Apple FS, Ler R, Murakami MM. Determination of 19 cardiac troponin I and T assay 99th percentile values from a common presumably healthy population. Clin Chem. 2012;58(11):1574–1581; doi: 10.1373/clinchem.2012.192716.
- Bonaca MP, O’Malley RG, Jarolim P, et al. Serial cardiac troponin measured using a high-sensitivity assay in stable patients with ischemic heart disease. J Am Coll Cardiol. 2016;68(3):322–323; doi: 10.1016/j.jacc.2016.04.046.
- Ford I, Shah ASV, Zhang R, et al. High-sensitivity cardiac troponin, statin therapy, and risk of coronary heart disease. J Am Coll Cardiol. 2016;68(25):2719–2728; doi: 10.1016/j.jacc.2016.10.020.
- Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. J Am Coll Cardiol. 2014;64(24):e139–e228; doi: 10.1016/j.jacc.2014.09.017.
- Bonaca MP, Ruff CT, Kosowsky J, et al. Evaluation of the diagnostic performance of current and next-generation assays for cardiac troponin I in the BWH-TIMI ED chest pain study. Eur Heart J Acute Cardiovasc Care. 2013;2(3):195–202; doi: 10.1177/2048872613486249.
- Schreiber DH, Agbo C, Wu AHB. Short-term (90 min) diagnostic performance for acute non-ST segment elevation myocardial infarction and 30-day prognostic evaluation of a novel third-generation high sensitivity troponin I assay. Clin Biochem. 2012;45(16–17):1295–1301; doi: 10.1016/j.clinbiochem.2012.06.005.
- Schofer N, Brunner FJ, Schlüter M, et al. Gender-specific diagnostic performance of a new high-sensitivity cardiac troponin I assay for detection of acute myocardial infarction. Eur Heart J Acute Cardiovasc Care. 2017;6(1):60–68; doi: 10.1177/2048872615626660.
- Sgx Clarity cTnI assay: instructions for use. Alameda, Calif: Singulex, 2017.
- Rozanski A, Gransar H, Hayes SW, et al. Temporal trends in the frequency of inducible myocardial ischemia during cardiac stress testing: 1991 to 2009. J Am Coll Cardiol. 2013;61(10):1054–1065; doi: 10.1016/j.jacc.2012.11.056.
- Adamson P, Hunter A, Shah A, et al. High-sensitivity cardiac troponin I and the diagnosis of obstructive coronary artery disease in patients with suspected stable angina. J Am Coll Cardiol. 2017;69(11 Supp):19; doi: 10.1016/S0735-1097(17)33408-3.
- Gaïni S, Koldkjaer OG, Pedersen C, Pedersen SS. Procalcitonin, lipopolysaccharide-binding protein, interleukin-6, and C-reactive protein in community-acquired infections and sepsis: a prospective study. Crit Care Lond Engl. 2006;10(2):R53; doi: 10.1186/cc4866.




{kind=link}