
 |
HIV infection and AIDS are among the leading causes of illness and death in the United States. According to the Centers for Disease Control and Prevention (CDC), by 2004, nearly 1 million people were diagnosed with AIDS; 50% of them succumbed to the disease. In 1995, highly effective antiretroviral therapy (HAART) was introduced. The annual number of AIDS cases and deaths declined substantially and stabilized between 1999 and 2004. However, since 1994, cases increased among African Americans, racial/ethnic minorities, and persons exposed via heterosexual contact.
The CDC enhanced HIV testing guidelines with increased screening options, counseling, and detection assay options for labs. With increased screening and diagnostic tests for HIV-infected pregnant women followed by increased antiretroviral prophylaxis efficacy, mother-to-child HIV transmission reduced from 95% (in 1992) to 48% (in 2004).
In 2006, many barriers to HIV early detection and treatment were removed by the CDC with a new guideline for HIV detection tests to be considered for all patients age 13 to 64 years, regardless of risk, with an opt-out screening option and focused testing guidelines.
In the nearly 3 decades since the discovery of the AIDS virus, molecular techniques and infectious disease diagnostics have been put in place; and medical and CDC professionals, and World Health Organization (WHO) members, have worked aggressively to have a global consensus on HIV awareness, detection, treatment, and counseling. Initial focus is on detection, which started with HIV antibody detection in patient samples, followed by counseling and treatment.
 |
HIV Screening Tests: Reasons, Results, and Ramifications
After the discovery of the AIDS virus and the announcement of stringent HIV testing in blood banks in 1984, the first antibody testing for HIV began in 1985 with the introduction of an enzyme immunoassay, or EIA, for screening of donated blood. The idea behind blood screening was:
- To protect blood supplies with high sensitivity;
- To be suitable for batch processing of high specmen volumes; and
- To provide accurate results in a short time.
With further investigations, a two-test sequential algorithm was established: an EIA screening followed by a Western blot as confirmation. While this two-test algorithm became the “gold standard,” certain disadvantages of the methodology were also determined. EIAs are technically challenging and require sophisticated lab equipment with a constant electric supply. Efficient EIA usage also requires at least a 96-well setup per run. Therefore, in developing and underdeveloped countries and in smaller labs, such testing would require more money and time.
In addition, Western blots include high-cost, well-trained technicians, with a high probability of indeterminate results. Therefore, a combination of the above techniques and new ones was devised to be used in HIV screening in an economical, fast, and reliable fashion. Some techniques are:
ELISA tests: Screening antibodies reacting to the presence of the HIV antigen. Highly sensitive, these tests weren’t as specific as required. However, the p24 antigen ELISA test detected the p24 surface protein without requiring an antibody response and is considered in conjunction with a Western blot for confirmatory purposes.
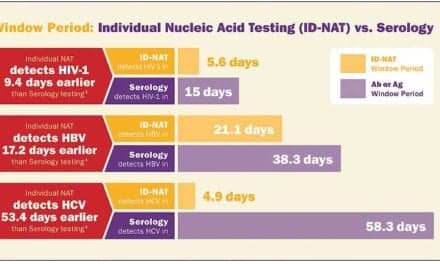
NAT: Nucleic Acid Tests (NATs) allow for the detection of the genetic material and are much more specific and sensitive than immunoassays, using transcription-mediated amplification (TMA) or polymerase chain reaction (PCR). These tests are more expensive and require those with technical know-how to run them.
Rapid tests: Rapid point-of-care tests (POCTs) are used for initial screening and are encouraged in high-prevalence regions as they require less instrumentation, handling, time, and lab setup.
NAT Tests for HIV Screening
Gen-Probe, San Diego, a global leader in the world of rapid, accurate, and cost-effective NATs, released the APTIMA HIV-1 RNA Qualitative Assay—the first FDA-approved NAT test for HIV-1 detection in human plasma—in 2002. The assay is used specifically for diagnosis of acute or primary HIV-1 infection, which is indicated by the presence of HIV-1 RNA in patient plasma samples. A collaboration between Chiron (a Novartis business) and Gen-Probe proved to be very successful with the PROCLEIX HIV 1/HCV assay, currently used in the United States to screen more than 80% of donated human blood annually.
Measurement of blood plasma HIV-1 RNA concentration, or “viral load,” using NAT is the standard of care around the world. Since untreated HIV-1 infection yields high viral production and loss of CD4 T-cells (despite a lengthy clinical latency lag), the US Department of Health and Human Services advocates use of viral-load testing during HAART. In addition to the TMA employed in the Gen-Probe tests, other viral load assay manufacturers focus on PCR-based amplification techniques.
ELISA-Based Rapid Point-of-Care Tests
Although the initial ELISA tests followed by confirmatory Westerns or EIAs are still prevalent and conclusive for HIV testing, the ELISA test has undergone several iterations that can be conclusive, relatively inexpensive, and quick. Kalpana Natrajan, MD, of the Pulmonary Medicine and Infectious Disease Medical Group at Sharp Grossmont and Scripps Mercy hospitals, San Diego, explains her concern. “As an infectious diseases’ doctor, I require that AIDS screening/testing kits are both sensitive and specific. She adds that a quick turnaround time is important, since, she says, “Waiting for such results can be very stressful for a patient.”
To that end, rapid tests have filled an essential space in HIV testing. Some of the formats include: lateral flow, in which the blood sample migrates through a nitrocellulose membrane, yielding a detection signal in less than 15 minutes (this test is the latest in rapid tests, least expensive, reliable, and does not require additional manipulation or refrigeration); and flow-through cassettes that capture and detect HIV antibodies in a specimen flowing through a porous membrane (reagents require multiple washes and refrigeration).
Other tests include solid-phase tests, which could be the dipstick “comb” assay, in which a solid plastic matrix contains the HIV antigen and if the corresponding antibody is present in the specimen, a dot will appear on the matrix. Finally, there is the agglutination test, in which different clumping particles are used to test a specimen that will clump, settle, or aggregate based on the presence of HIV antibodies (requiring refrigeration, as introduced inaccuracies may lead to subjective interpretation of these tests).
At the 2008 International AIDS conference in Mexico City, Inverness Medical, San Diego, launched the fourth-generation rapid Determine HIV Ag/Ab Combo test. Capable of detecting HIV infection days earlier than an antibody-only test, the test combines the simultaneous detection of HIV p24 antigen and antibodies for HIV 1 and 2 in human blood, serum, and plasma.
Bio-Rad, Hercules, Calif, another leader in clinical diagnostics rapid assays, has among its latest tests the Multispot HIV-1/2 Rapid Test. Classified as a CLIA-moderately complex test, it is the first test for use in the United States for both fresh and frozen plasma and serum as a rapid, indirect EIA test.
CD4 T-cell Count-Based Rapid Tests
The need for rapid tests is obvious: easy to use, quick, accurate detection, little hands-on time, and easy readouts. All these tests focus on antibody-detection or p24 antigen, or a combination of both. But what about absolute CD4 T-cell counts? Rajeev Jairam, MD, FRANZP, resident MD, Scripps Mercy Hospital, considers that very important. “Such a kit will expedite the treatment process for the doctors and the patient.”
PointCare Technologies, Marlborough, Mass, has the PointCare NOW kit monitoring CD4 T-cells for patient management. With results obtained in less than 8 minutes, this is fully automated from start to finish, with long shelf-life reagents requiring no special handling. It measures both absolute and lymphocyte percentage CD4 T-cell results, which allow physicians to start a treatment regimen for patients in a single visit. An RN or a phlebotomist under low-throughput and limited clinical lab resources can draw 2 mL of blood for the test and read the results in real time.
Recent Advances: HIV-1 Diagnostic Testing
While most companies agree that a specific and directed test is most needed for HIV testing, real-time PCR assays come close to fitting the bill. The advantages of using real-time PCR are the maintenance of sensitivity and specificity of end-point PCR, added to which is a significantly extended linear dynamic detection range (~5-log). Some examples include the COBAS AmpliPrep/COBAS TaqMan HIV-1 test from Roche Diagnostics, Indianapolis, that uses primers and probes to amplify the HIV-1 gag sequence (if present) in postsample prep in a 48-sample analyzer.
While real-time assays show great promise, with greater detection ranges, specificities, and sensitivities, the cost of an assay as well as its ease of use are the concerns in running such tests. Additionally, real-time assays can definitely be advantageous compared to Westerns in terms of time and results.
Future of Screening Tests
The future of HIV screening tests appears to be the same for clinicians as well as diagnostics companies: rapid tests. “Prior to the advent of rapid testing, the turnaround time for an HIV EIA in our hospital was approximately 3 days,” Jairam says. “The turnaround time [even] on a PCR in the setting of suspected acute HIV infection is still slow and can affect treatment.”
He and many in the field feel that the test for patients should be rapid, specific, sensitive, and, of course, cost-effective. Natrajan agrees that the stigma associated with being tested causes many patients to not seek treatment at all. Additionally, according to Natrajan, “In the near future, a kit that detects drug resistance in HIV in a rapid fashion would be very useful to doctors.”
These are steps beyond diagnostics products, in that, once these diagnostic tests are used for detection, proper drug therapy should be initiated rapidly. Another area of concern for clinicians is that these rapid tests be administered in a doctor’s office easily. Natrajan firmly believes that patients would be more willing to be tested for HIV in an environment that is comfortable for them, such as the doctor’s office under low-throughput conditions. “By testing in the office, doctors will be able to identify and treat new cases of HIV sooner … and therefore provide better quality of care and help prevent the spread of HIV,” she says.
Currently, most clinicians order lab tests that are either EIAs or ELISAs followed by Western blots for confirmation purposes even if they take longer than rapid tests. Why is that? “I rarely order rapid tests unless I am meeting a patient in the outpatient setting for the first time and I think they may not follow up as planned,” Jairam notes. “The ER is probably the best setting for rapid tests as patient follow up is never guaranteed.”
This may be an interesting observation for diagnostic companies to note that clinicians prefer to wait a few weeks to get confirmatory tests rather than rapid tests unless the need is immediate for a high-risk patient in emergency-department conditions. The future of such screening obviously lies in continuous cross-communication between physicians, medical professionals, clinical diagnostics companies, and the government regarding assay benefits, uses, cost, and efficiency of these tests. But most clinicians and scientists agree that HIV testing should become accepted as a “routine screening test,” similar to a mammogram, colonoscopy, or PSA.

To stay current on HIV testing methods, bookmark our website. |
The challenges that diagnostic companies face are many. Some of them include adoption of point-of-care products by physicians and clinical labs; standard insurance reimbursement issues; the fact that some states still require informed consent; and sample-collection requirements in some states, such as California, where a licensed phlebotomist is needed to perform a finger-stick test.
With the urgent need of HIV testing to be easily accessible, sensitive, specific, and cost-effective, now is the time for clinicians, medical labs, and diagnostics companies to take this opportunity to drive HIV testing forward—not only for screening blood in blood banks, but individual patient samples for a quicker turnaround, a faster treatment schedule, and a reduction in the further transmission of the virus.
Madhushree Ghosh, PhD, is a contributing writer to CLP.
Recommended Reading
Branson BM. Point-of-care rapid tests for HIV antibodies. J Lab Med. 2003;27(7/8):288-295.
Branson BM, Handsfield HH, Lampe MA et al. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR Recomm Rep. 2006 Sep 22;55(RR-14):1-17; quiz CE1-4.
Swanson P, de Mendoza C, Joshi Y et al. Impact of human immunodeficiency virus type 1 (HIV-1) genetic diversity on performance of four commercial viral load assays: LCx HIV RNA quantitative, AMPLICOR HIV-1 MONITOR v1.5, VERSANT HIV1 RNA 3.0, and NucliSens HIV-1 QT. J Clin Microbiol. 2005;43(8):3860-3868.
APTIMA HIV-1 RNA Qualitative Assay. Available at: [removed]www.gen-probe.com/products/aptima_hiv.aspx[/removed]. Accessed April 7, 2009.
Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health care settings. Available at: www.cdc.gov/mmwr/preview/mmwrhtml/rr5514a1.htm. Accessed April 7, 2009.



{kind=link}