
Increasing public awareness of the laboratory’s role in public health offers an opportunity to slow the spread of sexually transmitted infections.
By Lauren Albrecht, MPH, MLS (ASCP)cm
The covid-19 global pandemic has turned an unprecedented spotlight on the importance of public health. Suddenly, people are regularly hearing news stories about the laboratory’s role in the pandemic response, and testing for the disease is a topic at dinner tables across the country—which is exciting for the laboratorians who are used to their career choice being misunderstood, if acknowledged at all.
The laboratory community can take advantage of this newfound appreciation for our profession. Clinical laboratorians play an important role in public health, and the laboratory community has an opportunity to build on that momentum to help keep the focus on important public health matters that will still be around once covid-19 cases start to diminish. Beyond pandemic response, laboratory work is critical to the control of smaller outbreaks and epidemics, like the ever-increasing cases of sexually transmitted infections (STIs).
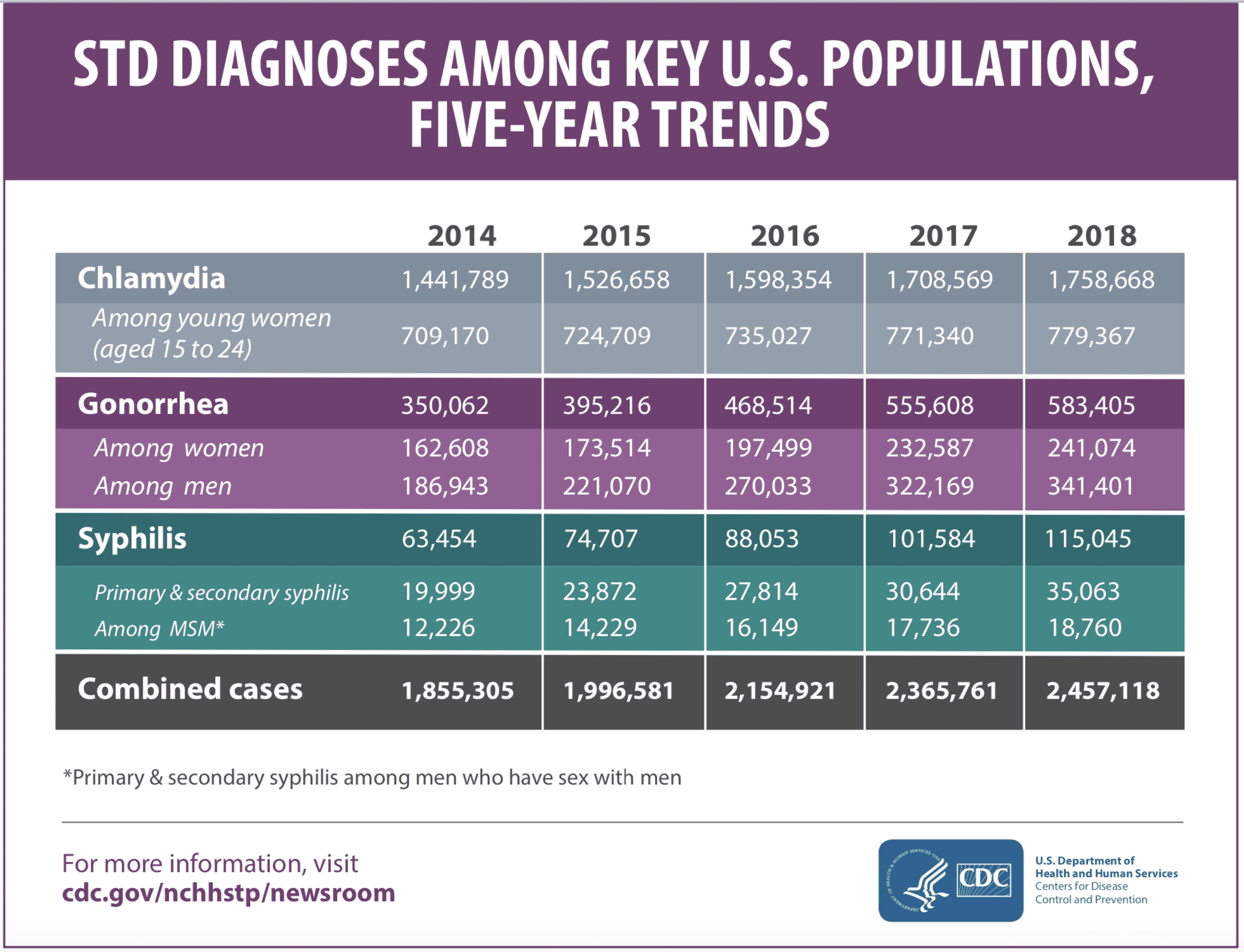
The year 2018 marked an all-time high for reportable cases of STIs, according to the Centers for Disease Control and Prevention (CDC) 2018 STD Surveillance Report.1 Highlighted within the surveillance data is evidence of an alarming rise in the incidence of all STIs: Since 2014, cases of chlamydia have increased 19%, cases of gonorrhea have increased 63%, and primary and secondary syphilis cases have risen a massive 71% (Figure 1). To address these rises, the US Department of Health and Human Services included targets for this epidemic in the Healthy People 2020 (HP2020) initiatives, but many people, including laboratorians, are not aware of this program. And so the targets to reduce gonorrhea rates—and to reduce sustained domestic transmission of primary, secondary, and congenital syphilis—were nowhere close to reaching their targets by the end of 2020. Laboratories from all over the country are a huge part of this system that creates useful data to track and follow disease trends that helped shape the goals of HP2020 and will lead to the changes that will be made for Healthy People 2030 initiatives.
The emergence of covid-19 has also brought the term “epidemiologist” further into the public vernacular, and this group of public health officials will continue to work on the STI issue long after media attention shifts away from the pandemic. Epidemiologists are responsible for the everyday tracking of incidence and prevalence of disease to help come up with objectives to decrease these rates through public health interventions in the areas that need it the most. The current spotlight on laboratories and public health may not last, but we can use this moment to educate the public about how the health system works in this country and bring to light the ongoing efforts and goals of the laboratory community in controlling other diseases, like the spread of STIs.
Rising Incidence of STIs
This rise in STI incidence may be surprising to some, and it can be attributed, but not limited to, the lack of access to healthcare in underserved populations and a weakened public health infrastructure. For many people, especially the younger generation, barriers to finding out their disease status includes a lack of knowledge of STIs and available services, long wait times, conflicts between clinic hours and personal schedules, the embarrassment attached to seeking services for STIs, and the method of specimen collection. These barriers are especially problematic when it comes to the regular screening of asymptomatic young adults.2 Men who have sex with men (MSM) have a higher incidence of STIs than any other group and are similarly unlikely to seek appropriate screening due to similar barriers as listed above.
Another factor contributing to the rise in cases is that most people who experience STIs do not present with any symptoms—when symptoms do occur, they can easily be mistaken for those caused by urinary tract infections (UTIs). A study performed in an urban academic emergency department collected data on women with genitourinary symptoms and found that 64% of the patients with a missed STI were diagnosed as having a UTI instead.3 Once diagnosed, current guidelines also suggest repeat testing 3 months after treatment to ensure that treatment was successful.4 Unfortunately, poor adherence to these guidelines contributes to the spread of these diseases among higher-risk populations.
The cost of an undiagnosed and untreated STI is high: When left untreated, STIs can lead to pelvic inflammatory disease, inflammation, and infertility. The economic costs of these infections can be estimated upward of $17 billion per year depending on the model used and the outcomes that are measured.5 Most of the direct costs of STIs are due to a failure to detect and effectively manage the disease in its initial acute stage. One example is chlamydia—which alone accounts for yearly costs of $1.5 billion, nearly three-fourths of which is due to preventable complications resulting from untreated and initially uncomplicated infections.5 The costs, both to the economy and to the health of our communities, should be argument enough that screening, especially in high-risk populations, needs to be a top priority in healthcare and public health settings.
Emerging Issues
While the best known STIs are increasing in prevalence, a few more “bugs” have been emerging and becoming a concern.
Mycoplasma genitalium, for example, has been linked to urethritis in men but has a less definitive pathogenic role in women. Data is scarce, but it may be responsible for up to 15% to 20% of nongonococcal urethritis (NGU) cases, 20% to 25% of nonchlamydial NGU cases, and about 30% of the instances of persistent or recurrent urethritis.4 This pathogen is more common than infections with Neisseria gonorrhoeae but less common than Chlamydia trachomatis in most settings. In women, M. genitalium can be detected in the vagina, cervix, and endometrium, but these patients mostly present as asymptomatic, and overall the organism seems to have less of a definitive pathogenic role.4
While research on M. genitalium shows that this infection could lead to pelvic inflammatory disease and infertility in women, nothing is definitive enough to make a direct connection. This organism is slow growing and can take up to 6 months to grow in a culture. Because of this, the standard of testing for it is a nucleic acid amplification test (NAAT). Thankfully an FDA-approved NAAT for M. genitalium entered the market in January of 2019: The Aptima Mycoplasma genitalium assay can be used with urine or with urethral, penile meatal, endocervical, or vaginal swab samples collected in a clinical setting.6 With more commercial testing and awareness of M. genitalium’s role in STIs, research can be done to fill in the gaps that we currently have.
While hepatitis C (HCV) is the most common chronic bloodborne infection in the United States, new data suggests that sexual transmission of HCV is also a problem, especially among MSM with concurrent HIV infections. New York City, Boston, and multiple European cities have reported an increasing incidence of acute HCV infection among this population.4 Many people who become infected with HCV can be asymptomatic or present with a mild clinical illness, which means that there may be a long time between infection and diagnosis, increasing the chances that these individuals may unknowingly spread it to others. However, with screening, HCV RNA can be detected in blood as early as 1 to 3 weeks after exposure, and anti-HCV can be detected in over 97% of infected persons 6 months after exposure.4
The CDC has recently changed its HCV screening guidelines by adding an HCV screening at least once in a lifetime for all adults 18 years and older, except in settings where prevalence of HCV infection is less than 0.1%. They also recommend HCV screening for all pregnant women during each pregnancy, except in settings where the prevalence of HCV infection is less than 0.1%.7 Since it has been noted that HCV can be recovered from the semen of men with HIV, special care to include this information while consulting with high-risk patients should be made a priority, along with a discussion on prevention practices such as using barrier precautions to limit transmission during sexual contact.
Thanks to the availability of rapid NAAT for STI testing, specifically for gonorrhea, fewer laboratories are actually growing N. gonorrhoeae in culture. With no culture, we lose the ability to perform any antimicrobial sensitivity testing, an issue that has led to the emergence of antibiotic-resistant gonorrhea. The CDC recommends that for any N. gonorrhoeae infection that does not respond to cephalosporin treatment, the patient should have a specimen taken for culture and antimicrobial susceptibility testing, which will need to be reported to the CDC through state and local public health authorities.4 Since a number of laboratories no longer perform cultures, due to the cost and the logistics of handling and incubating growth media, a mechanism needs to be in place to initiate this testing if a laboratory performs only NAAT testing for gonorrhea.
The Laboratory’s Role
The country (and the world) has made it a top priority to slow the spread of covid-19. But laboratorians and healthcare providers can use lessons learned from the pandemic to help slow the spread of rapidly increasing STIs. It is clearer than ever that a strong public health infrastructure is needed to help combat disease, especially in areas of greater need. Using covid-19 as an example, it is easy to see how an airborne virus primarily affects highly populated cities rather than the rural parts of a state where there is less contact between individuals.
For STIs, it is not population density that is directly correlated to prevalence; instead, areas with STI outbreaks are generally at higher risk due to social, economic, and behavioral factors. Therefore, epidemiologists involved in STI research focus more on how certain racial and ethnic groups have higher rates of STIs, how poverty leads to disproportionate rates of disease, and how marginalization leads to less access to healthcare and less health-seeking behavior. They also study how substance abuse behaviors can help spread the epidemic; how social factors can lead to a stigma attached to STIs, making it uncomfortable to talk about sex-related behaviors; and how sexual networks contribute to the spread.
“Contact tracing” is another new epidemiological buzzword that has taken hold within the general population during this pandemic. With covid-19, the idea is to use test results to encourage self-isolation for anyone who has come into contact with a person who has a confirmed case. A similar idea with STIs is called expedited partner therapy (EPT), defined as “treating the sex partners of persons with sexually transited diseases without an intervening medical evaluation or professional prevention counseling.”10 This means that when a person is diagnosed with an STI, their sexual partner(s) can also receive treatment immediately, without needing to see a doctor or be tested themselves. The CDC gives guidance on EPT for each specific disease, and as of May 2020 EPT is permissible in 45 states, potentially allowable in four others, and is currently prohibited only in South Carolina. The best way to help slow the spread of diseases that are passed along through sexual contact is to also treat the partners of the patients who are diagnosed.
Finally, there is wide public acknowledgement of the need to screen asymptomatic populations in the fight against covid-19. While guidelines for this goal are still under construction, asymptomatic screening of population for STIs does exist and has for some time. With the prevalence of asymptomatic carriers for most STIs, the need for screening is very important. However, compliance with these testing guidelines can be low, with populations in need falling through the cracks due to the barriers discussed previously.
Luckily, with the rise in NAAT testing for STIs, less invasive sample collections have become an option, along with the use of urine as a specimen instead of direct genital swabs. These sampling techniques have a major advantage because they are noninvasive and can be collected in areas outside of a doctor’s office. Companies such as BD Max, Hologic, and Cepheid have FDA-approved STI testing that can be performed on patient-collected vaginal swabs in clinical settings. A meta-analysis has shown that participants were three times as likely to get tested for any STI when using a self-collection method when compared to clinician collection.8 In addition, some manufacturers have testing approved for extragenital specimens. The Aptima Combo 2 Assay and the Xpert CT/NG Assay allow for the use of throat and rectum sample collection for both chlamydia and gonorrhea testing.9
Some home collection kits have been approved through the emergency use authorization (EUA) for covid-19, and several of the companies selling them also offer home collection kits for STIs. While these collection techniques are not approved by the FDA, some laboratories may use these samples for testing in high-complexity settings where they have extensively validated test performance as laboratory-developed tests. While at-home testing collection kits could be the answer for overcoming so many barriers that exist for standard STI testing, a patient needs to be wary and make sure that the test kits are going to a CLIA-certified laboratory for testing. Any laboratory performing testing using a method that is not FDA approved (such as using a nonapproved collection method with an FDA-approved test method) must perform extensive validation procedures to ensure accuracy. Because they are modifying the specimen type and/or mode of collection, they are using the test outside of the manufacturer’s instructions. Besides assessment of accuracy, precision, limit of detection, and any possible interfering substances, the laboratory must also validate the stability of samples through transport and storage. The collection instructions for a home-collection kit should also be written to ensure the consumer’s compliance on arguably the most important step of all laboratory testing: obtaining an appropriate specimen.
While some laboratories are equipped to establish their own in-house methods, the gold standard for most laboratories will always be FDA-approved testing, performed with the approved collection technique, using the assay’s approved method. Currently, however, there is only one at home HIV-testing kit that has been approved by the FDA. The OraQuick in-home HIV test is available for purchase, and the CDC has more information on the uses for this test.
Laboratory testing has been rapidly evolving the past few years, and while some of it is breaking into new territory that may make some traditional laboratorians cringe at the “what-if” scenarios, the new collection methods being developed can go a long way toward counterbalancing the barriers to testing that many patients face.
Conclusion
The covid-19 pandemic has been an eye-opening experience; let us hope that it has shown more people just how important public health is to our everyday lives in America—and how important is the work of all the laboratorians working silently behind the scenes. Epidemiologists and laboratorians are both necessary in the fight against covid-19, but as the pandemic fades they will be equally important in the fight against the huge rise in incidence of STIs.

While laboratorians do not directly work with epidemiologists in most cases, the test results and demographic data collected by laboratories are critical for any public-health response, and epidemiologists use this data every day. The laboratory is critically important in the health of the community as a whole, whether the problem is a pandemic or another transmissible disease like an STI. With the newfound attention this pandemic has turned onto laboratorians, we hope to see more attention paid to the shortage of lab professionals in this country. And solving that problem will help us to continue limiting the spread of disease, one test at a time.
Lauren Albrecht, MPH, MLS (ASCP)cm, has six years of clinical laboratory experience, most of which she spent working in the blood bank at University Hospitals in Cleveland, Ohio. She went on to receive an MPH in epidemiology at Kent State University to help supplement her Medical Laboratory Scientist certification. Currently she is a COLA surveyor where she has been educating and helping laboratories follow CLIA regulations for the past three years in the Midwest and on the East Coast.
References
1. Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2018. Atlanta: U.S. Department of Health and Human Services; 2019. doi: 10.15620/cdc.79370.
2. Tilson EC, Sanchez V, Chandra CL, et al. Barriers to asymptomatic screening and other STD services for adolescents and young adults: focus group discussions. BMC Public Health. 2004;4:21 doi: 10.1186/1471-2458-4-21.
3. Tomas ME, Getman D, Donskey CJ, Hecker MT. Overdiagnosis of urinary tract infection and underdiagnosis of sexually transmitted infection in adult women presenting to an emergency department. J Clin Microbiol. 2015;53(8): 2686-2692. doi:10.1128/jcm.00670-15.
4. Workowski KA, Bolan GA, Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR-03):1–137. pmid:26042815.
5. Eng TR, Butler WT, eds, Institute of Medicine (US). Summary: The Hidden Epidemic: Confronting Sexually Transmitted Diseases. Washington, DC: National Academy Press; 1997.
6. FDA permits marketing of first test for STI caused by Mycoplasma genitalium. Infection Control Today. January 28, 2019. Available at: https://www.infectioncontroltoday.com/view/fda-permits-marketing-first-test-sti-caused-mycoplasma-genitalium. Accessed February 18, 2021.
7. Schillie S, Wester C, Osborne M, Wesolowski L, Ryerson AB. CDC recommendations for hepatitis c screening among adults — United States, 2020. MMWR Recomm Rep. 2020;69(2):1–17. doi: 10.15585/mmwr.rr6902a1.
8. Ogale Y, Yeh PT, Kennedy CE, Toskin I, Narashimhan M. Self-collection of samples as an additional approach to deliver testing services for sexually transmitted infections: a systematic review and metaanalysis. BMJ Glob Health. 2019;4(2):e001349. doi: 10.1136/bmjgh-2018-001349.
9. Food and Drug Administration. FDA clears first diagnostic tests for extragenital testing for chlamydia and gonorrhea [press release]. May 23, 2019. Available at: https://www.fda.gov/news-events/press-announcements/fda-clears-first-diagnostic-tests-extragenital-testing-chlamydia-and-gonorrhea. Accessed September 14, 2020.
10. Centers for Disease Control and Prevention. Expedited Partner Therapy in the Management of Sexually Transmitted Diseases. Atlanta, GA: US Department of Health and Human Services; 2006. Available at: https://www.cdc.gov/std/treatment/eptfinalreport2006.pdf. Accessed February 18, 2021.
11. Centers for Disease Control and Prevention. STD diagnoses among key U.S. populations, five-year trends. October 8, 2019. Available at: https://www.cdc.gov/nchhstp/newsroom/docs/factsheets/STD-Table-2018_Final.pdf. Accessed February 18, 2021.




{kind=link}