Flexible panel testing is the latest of many advances for the field
By Nikki Fette, MT(ASCP), CLS(NCA)

Nikki Fette, MT(ASCP), CLS(NCA), Parkview Medical Center.
Over the past 10 years, the practice of microbiology in the clinical laboratory has changed significantly. Formerly regarded as a field whose work was a slow-moving “art,” microbiology has recently taken on new life, evolving to become the focal point of a fast-paced stat environment.
In the past, clinicians did not expect to receive actionable results from the microbiology lab because of the prolonged turnaround times associated with culture-based diagnostics, which can take anywhere from 4 to 9 days to produce definitive results. Arriving long after any meaningful window for therapeutic decisionmaking had already closed, unfortunately, such results were often viewed by clinicians as merely confirmatory.
With the development of molecular diagnostics using polymerase chain reaction (PCR) technologies, however, clinically meaningful patient results for infectious disease testing are now widely available in just a matter of hours. Moreover, related advances have reduced the complexity of such molecular tests, making them both more affordable and simple enough to be performed in all clinical microbiology laboratory settings.
In turn, the adoption of such diagnostics has increased the interaction of laboratorians with other key stakeholders in the hospital. Studies have demonstrated that implementation of molecular infectious disease tests can significantly improve patient outcomes and decrease overall costs for the patient and hospital. Microbiology departments that are able to make such contributions are now being encouraged to work closely with infectious disease clinicians and pharmacists to develop innovative antibiotic stewardship strategies aimed at saving patient lives, reducing unnecessary treatment costs, and better controlling the spread of antimicrobial resistance.
Achieving these goals can be vital for ensuring that community hospitals and their laboratories will survive, especially in a time when Medicare and Medicaid reimbursement rates are being reduced year after year. While the changing healthcare environment may at times seem worrisome, laboratorians are doing their part to work efficiently and with fewer available resources to satisfy the needs of the providers and patients they serve.
TRADITIONAL TESTING FOR RESPIRATORY PATHOGENS
For clinicians who are trying to diagnose and determine treatments for their patients, respiratory pathogens are an enigma. The clinical symptoms related to such infections are often very generic, leaving many clinicians performing “guesswork.” But while symptoms alone may not enable clinicians to determine optimal patient management, factors derived from a patient’s medical and social history can guide them toward appropriate test ordering for a given patient.
Clinician ordering patterns are influenced by a number of factors, including seasonality, positivity, patient demographics, and turnaround time. For a patient population composed of adult outpatients during peak flu season, for instance, clinicians often order testing only for influenza and respiratory syncytial virus (RSV), as these are the clinically meaningful pathogens most likely to affect patient management decisions. For a higher-risk patient population, by contrast, clinician test ordering might favor a wider range of respiratory pathogen tests, as positive identification of an uncommon respiratory pathogen would have greater potential to affect patient management and cohorting decisions.
Over time, respiratory pathogen testing has evolved to better satisfy the needs of healthcare providers. (For more information, see the companion article, “Nonmolecular Methods for Respiratory Pathogen Testing.”) The original gold standard diagnostic for the detection of respiratory viruses was viral culture (traditional and shell vial). Such testing offers high sensitivity, but performing it is expensive, requires the work of highly skilled laboratorians, and may take 4 to 9 days to generate a definitive result. Most labs were not equipped to perform this type of testing because of their space limitations, financial limitations, or a shortage of qualified staff. As a result, they would often have to send out respiratory samples to a reference laboratory, thereby prolonging turnaround times even further beyond what could be considered a clinically actionable timeframe.
To address the limitations of viral culture, researchers developed antigen-based testing methods that can provide significantly shorter and more clinically meaningful turnaround times. While admittedly faster, however, antigen-based tests are known to perform with poor sensitivity and specificity, especially when the prevalence of the target organisms is low. Flu and RSV antigen tests have performed variably, with lower (and sometimes higher) sensitivity and specificity, depending on whether they are used in the appropriate season. In some cases, a good clinician could better diagnose flu on the basis of the patient’s symptoms alone, than by relying on the variable performance of antigen testing.
EVOLVING MOLECULAR
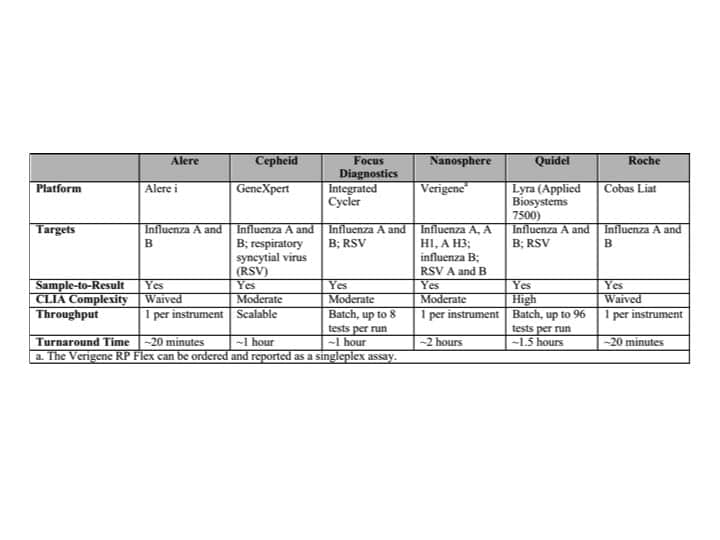
Table 1. Currently available molecular singleplex assays for respiratory pathogen detection. Click to expand.
Molecular applications for infectious disease testing began as “singleplex” tests, typically for one to four pathogens, and were based primarily on PCR methodology. Such early tests were designed to better address the limitations associated with culture-based diagnostics and generate accurate results that could be available in a clinically meaningful turnaround time. But while the first commercial PCR tests offered previously unrealized sensitivity for tests with faster turnaround times than culture, they were generally expensive, not fully reimbursable, and not always the easiest to perform in a lower skilled clinical laboratory setting.
Fluorescence in situ hybridization (FISH) is another singleplex molecular application developed for the clinical laboratory. FISH tests also provide accurate and relatively fast detection of pathogens for various disease states. But over time, FISH applications have been proven to require too much hands-on time for a busy stat microbiology and molecular environment.
Nevertheless, some institutions willingly lost reimbursement payments while implementing such exciting new testing platforms in attempts to improve patient care and decrease the patient’s hospital stay. (For more information, see the companion article, “Reimbursement for Molecular Respiratory Pathogen Testing.”)
Recently, researchers have developed multiplex PCR tests that can simultaneously test for 5 to 25 nucleic acid targets—a useful approach when clinical symptoms alone cannot narrow down testing needs to a smaller number of pathogens. Such “disease state” or “syndromic” panels are now available for a number of different infectious diseases. Performing such tests often requires as little as 2 minutes of hands-on time, with results available within 1 to 3 hours. Depending on clinician demand, the tests can be performed in batches or by random access. However, these tests also have limitations, as the number or type of pathogens tested can be too broad for some patients and too narrow for others.
CURRENT MOLECULAR TESTS
It was not until the development of singleplex and multiplex PCR respiratory pathogen tests that there was a viable solution that could provide the desired sensitivity and specificity in a turnaround time that was clinically meaningful to clinicians. There are now a handful of qualitative singleplex and multiplex platforms to choose from. These tests vary in pathogen coverage, workflow, cost, throughput, and turnaround time, but all seek to better meet the needs of providers by offering a diagnostic solution superior to culture and antigen-based methods.
Singleplex PCR solutions include tests from Alere, Cepheid, Focus Diagnostics, Quidel, and Roche, to name a few. Performed from nasopharyngeal swab specimens (NPS), these tests provide detection of influenza A, influenza B, or RSV in turnaround times ranging from 30 minutes to a few hours. Under the categories established by the Clinical Laboratory Improvement Amendments of 1988 (CLIA), they are either waived complexity and can be performed in point-of-care settings (Alere, Roche), or they are moderately complex and must be performed in a certified clinical laboratory (Cepheid, Focus, Quidel).

A Verigene system by Nanosphere, configured with two processors and one reader.
Broad respiratory pathogen testing options are provided by BioFire Diagnostics, GenMark, Luminex, and Nanosphere. These tests can detect 10 or more viral or bacterial pathogens simultaneously from nasopharyngeal swab specimens within a matter of hours. The respiratory panels by BioFire and Nanosphere are moderately complex sample-to-results tests, while the panels by GenMark and Luminex require offline extraction and amplification, and are categorized as high complexity.
When deciding which respiratory testing algorithms to offer, labs must of course consider the needs of the ordering healthcare provider. But they must also find a testing solution that provides their lab with the best performance, at the lowest cost, and with the most streamlined workflow. The selected respiratory testing algorithm should be affordable and easy to perform, with most community-based hospital laboratories requiring tests categorized as moderately complex or having waived complexity.
Quality control (QC) can be a huge cost issue when planning out molecular testing options, especially for supporting multiplex tests that require QC testing of rotating targets every 12 months. With a declining number of clinical laboratory scientists available, training and staffing can also become quite problematic, and is a major consideration for the adoption of any test. Space is another limitation of clinical laboratories. Many community hospitals don’t have the extra room to build their very own molecular section and are forced to squeeze in a few molecular instruments into a corner of the microbiology lab.
OBSTACLES AND ALTERNATIVES
For many labs, the current respiratory diagnostic solution is to choose between adopting multiple platforms; selecting a single abbreviated respiratory panel that does not provide comprehensive coverage and then sending the remaining respiratory orders to a reference laboratory; or running a one-size-fits-all respiratory pathogen panel that may be too broad for the patient population supported.
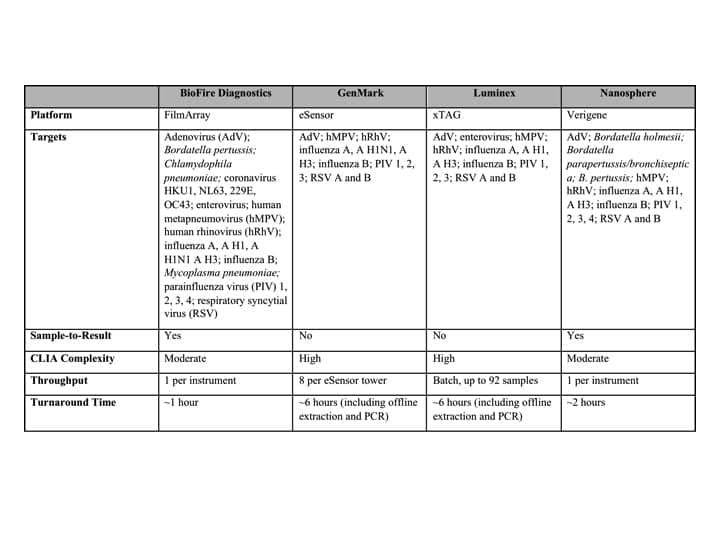
Table 2. Currently available molecular multiplex assays for respiratory pathogen detection. Click to expand.
Use of multiple platforms is too expensive for most laboratories and would place additional demands on lab personnel, including extra medical technician training, quality control testing, and proficiency testing. If labs decide to offer just one singleplex respiratory panel for influenza and RSV, they are left with few alternatives to sending out testing to a reference laboratory when a clinician requires additional pathogen testing. This algorithm is expensive and results in turnaround times that are not clinically actionable for a subset of respiratory specimen work-ups. Using a broad respiratory pathogen panel test often provides the necessary pathogen coverage. However, this approach either forces clinicians to order tests for targets not necessary for the patient, or forces laboratories to view and report results the clinician did not order. Such tests are expensive and can lead to unnecessary costs for the laboratory and the patient.
With reimbursement on the decline and a shift toward high-deductible healthcare plans under way, none of these options offers a sustainable, long-term solution. Such panels tests are often not customizable, and result in costly testing that is not always deemed necessary by public or private third-party payors.
While the diagnostic landscape for the detection of respiratory pathogens has advanced dramatically, no test yet exists that can address all the needs of clinicians and laboratorians at once. In a perfect world, the ideal respiratory pathogen test would be performed on a small, easy-to-use platform that is cost-effective, provides the necessary pathogen coverage, and is fully customizable to provider and patient needs.

The Verigene Respiratory Pathogens Flex test by Nanosphere employs a cartridge that contains a broad panel of 16 viral and bacterial targets.
An early attempt at achieving these goals is the Verigene Respiratory Pathogens Flex test (RP Flex) by Nanosphere. The RP Flex platform permits labs to select patient-customized subsets of targets from the 16 bacterial and viral pathogens on the panel, and to pay for only the targets reported. If the clinician requires additional testing, the lab can provide instant reflexing by making available previously unreported results from the original panel, without having to acquire a new patient sample or run an additional test. This approach will provide clinicians with more options, and will help laboratories to save on broad panels by limiting the reporting of information that is not clinically meaningful to all patients.
With such a test, labs can now offer testing for flu, flu and RSV, broad respiratory viral pathogen testing, and Bordetella pertussis testing, all on a single platform. In turn, labs will need to be concerned with only one instrument’s technician certifications, QC testing, proficiency testing, and inventory management. This type of flexible testing platform provides resource-limited community-based hospital labs with a means to offer a comprehensive respiratory testing algorithm that meets the needs of their providers and patients.
CONCLUSION
The challenges associated with the diagnosis and treatment of respiratory illness have diminished significantly over the past 10 years. This achievement is due to the improved quality, availability, and affordability of molecular diagnostic tests for clinical laboratories everywhere. Flexible molecular testing options such as Verigene RP Flex, however, could further advance the value of such diagnostics by responding better to the needs of the provider, patient, and lab. Such advanced performance will ultimately result in efficient and cost-effective patient care with meaningful results.
Nikki Fette, MT(ASCP), CLS(NCA), functions as the lead molecular technologist at Parkview Medical Center, Pueblo, Colo. For further information, contact CLP chief editor Steve Halasey via [email protected].



{kind=link}