
Diagnosis of C. difficile infection should be based on toxin detection
Johanna Sandlund, MD, PhD
The organism now known as Clostridiodes difficile—formerly Clostridium difficile—causes nosocomial and community-acquired gastroenteritis and is the most common pathogen leading to healthcare-associated infections.1 The clinical manifestations of C. difficile infection (CDI) range from asymptomatic carriage and mild diarrhea to toxic megacolon and death.2,3 Currently available tools used for the diagnosis of C. difficile infection lack in specificity, sensitivity, or turnaround time, leaving laboratorians, clinicians, and healthcare systems with complex, confusing, and costly solutions.
A Toxin-Mediated Disease
C. difficile was first described in 1935 by scientists studying the microbiota in infants.4 Due to culturing difficulties, the organism was named ‘difficile.’ There are two forms of C. difficile: a dormant, antibiotic-resistant spore-form; and a vegetative form with toxin-producing capability.5 Antibiotics can disrupt the normal intestinal flora and enable proliferation of C. difficile.2,3,6
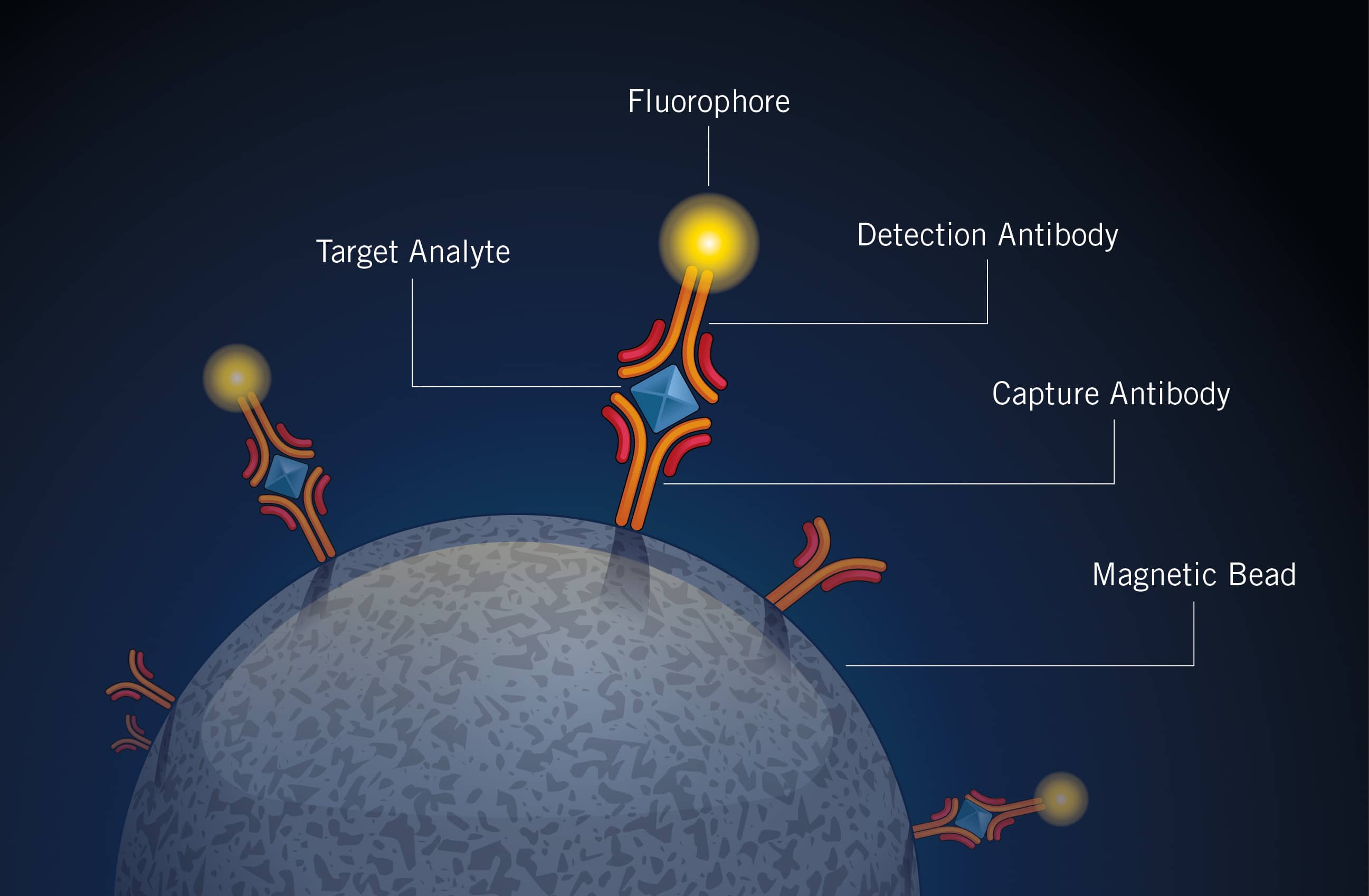
Figure 1. The proprietary single molecule counting technology from Singulex begins with one-step simultaneous binding of the analyte of interest to paramagnetic microparticles coated with capture antibodies and detection antibodies labeled with fluorescent dye.
The pathogenicity of C. difficile infection is mediated by two exotoxins, toxin A and toxin B, causing diarrhea and inflammation. The toxins have cytopathic effect and trigger structural and functional changes in host cells, such as cell rounding and blockage of Rho-dependent signaling.5,7 Diarrhea is likely a result of cytoskeleton disruption and increased epithelial permeability, and the loss of cell adherence leads to apoptosis.5,7 C. difficile toxins can also have cytotoxic effects, which lead to inflammation and colitis via inflammasome activation.5,7 Certain C. difficile strains produce a binary toxin, C. difficile transferase, which is associated with increased severity of C. difficile infection.5,7,8 Nontoxigenic strains—that is, those that do not produce toxins—are not considered pathogenic.5
C. difficile transmits via fecal-oral spread of spores at a very high rate, especially in healthcare settings, with the potential of causing outbreaks.5 Suspected and confirmed CDI cases are therefore subject to intense infection-control measures, including isolation.2,3 First-line therapy for C. difficile infection is antibiotics, which in and of itself increases risk for developing disease.3,9
The incidence and severity of C. difficile infection is rising.10 The emergence of more virulent strains has likely led to an increase in the number of CDI cases and also in severity of disease; changes in epidemiology, host response, and antibiotic pressure may also play a role in this progress.5 Asymptomatic colonization with C. difficile is also common; individuals can carry toxigenic C. difficile without having C. difficile infection.2,3,5,11
The Use and Misuse of Diagnostic Tests
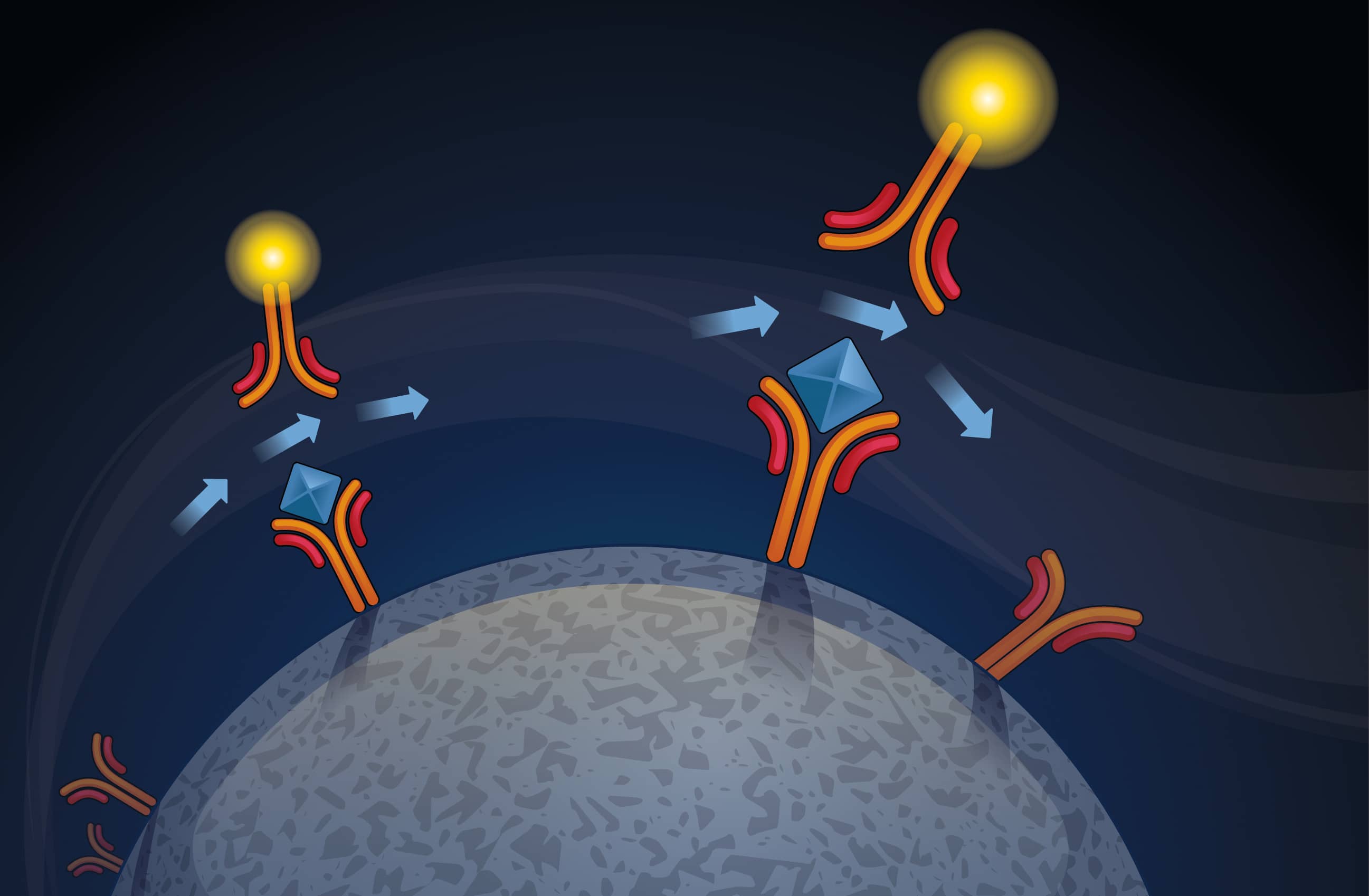
Figure 2. After incubation, the bound microparticles are washed to remove excess detection antibody and then subjected to conditions that disrupt the sandwich complex formed on the microparticles, creating an eluate.
The two reference tests for C. difficile infection—toxigenic cultures and cell cytotoxicity neutralization assays—are sensitive but take days to perform, leaving clinicians without timely, actionable laboratory results.
Up until recent years, the mainstay of CDI diagnostics was enzyme immunoassays for the detection of C. difficile toxins. However, such toxin enzyme immunoassays were known to lack sensitivity, and clinicians harbored a growing fear of missing cases. Attempts were made to increase sensitivity by adding testing for glutamate dehydrogenase (GDH), a C. difficile-specific antigen. However, tests for GDH do not differentiate between toxigenic and nontoxigenic strains of C. difficile.5,11
Concurrent with the initial reports of increasing incidence and severity of CDI cases, nucleic acid amplification tests were introduced in clinical microbiology laboratories. Molecular platforms and polymerase chain reaction (PCR) instruments for amplification of toxin genes offered a sensitive, automated, and rapid solution for CDI diagnostics. Most important, clinicians no longer had to worry about missing a case of C. difficile infection due to the poor sensitivity of enzyme immunoassays.
In addition, some PCR assays enable genotyping and detection of hypervirulent strains, such as 027/NAP1/BI.12 However, there is growing evidence to suggest that the role of 027/NAP1/BI in disease severity is minor in nonepidemic settings, and genotyping is not recommended in routine clinical laboratories diagnosing nonepidemic cases of C. difficile infection.13–15

Figure 3. The eluate containing fluorescently labeled detection antibodies is transferred to the plate and reader.
Unfortunately, nucleic acid amplification tests did not solve the problem of CDI diagnosis, but instead created another: overdiagnosis. PCR tests detect organisms with the capacity to produce toxins, but not the actual presence of the toxins.5,11 As a result, asymptomatic C. difficile carriers are diagnosed with C. difficile infection, placing a high burden on healthcare staff, hospitals, and long-term care facilities.6
The incidence of C. difficile infection is increasing, but likely in part due to poor test specificity.3,9 Unnecessary treatment. infection-control measures, and overreporting are harming patients, putting clinicians under pressure to lower reportable rates, and driving up costs for healthcare organizations.
Current Testing Recommendations
In the absence of feasible standalone assays for the diagnosis of C. difficile infection, the European Society of Clinical Microbiology and Infectious Diseases (ESCMID), the Infectious Diseases Society of America (IDSA), and the Society for Healthcare Epidemiology of America (SHEA) recommend using complex, multistep testing algorithms.3,9 ESCMID recommends combining sensitive and specific tests in two or even three steps.3 The IDSA/SHEA guidelines also recommend multistep algorithms, but accept standalone nucleic acid amplification testing if performed only on patients with a higher probability of C. difficile infection (ie, excluding stool specimens from patients receiving laxatives and with less than three unformed stools in 24 hours).9
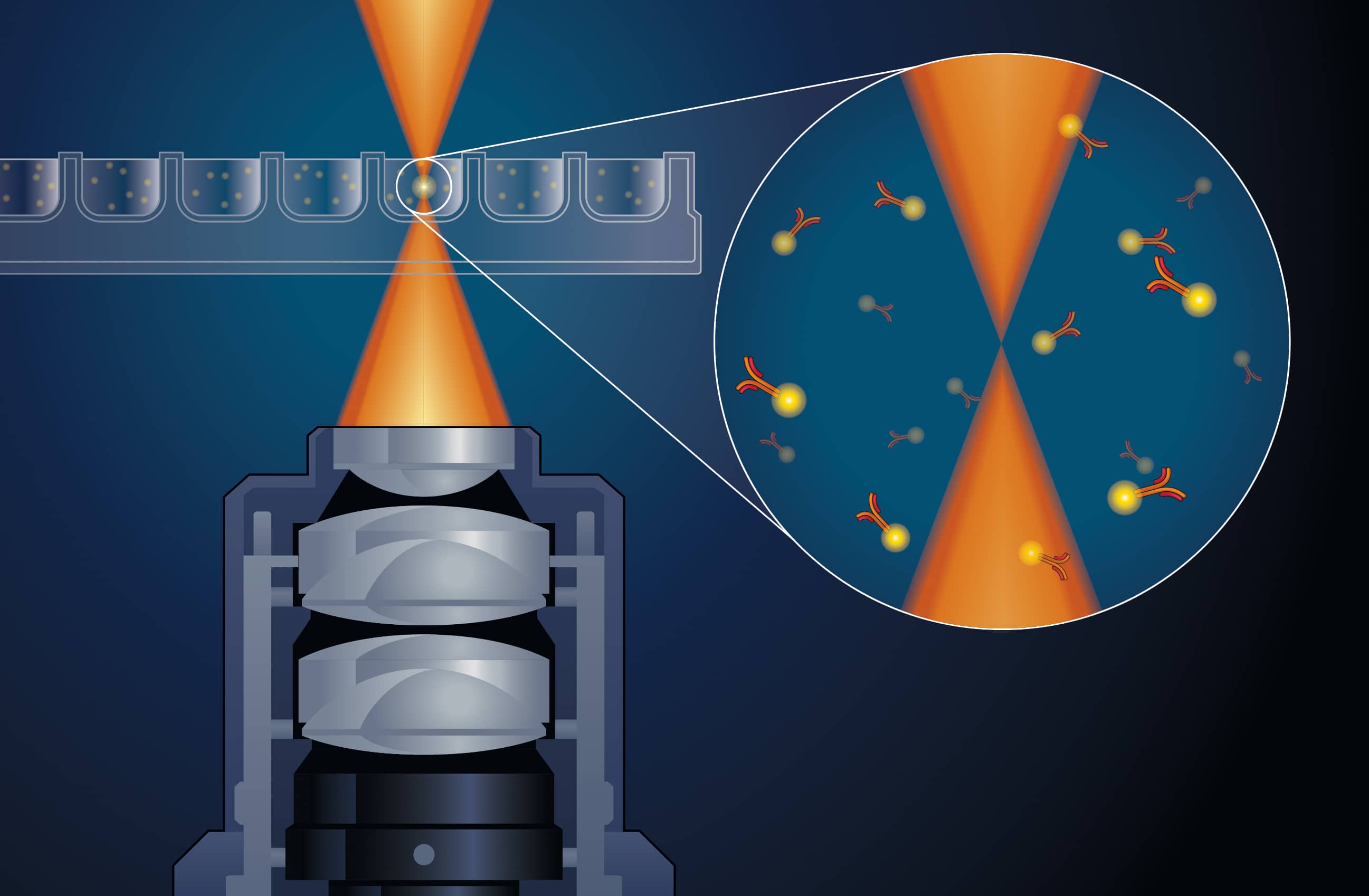
Figure 4. Digital counting is achieved using confocal optics focusing on a 5?m interrogation space, where fluorescently labeled molecules generate intense flashes of light as they are illuminated by a laser.
There is increasing evidence supporting a crucial role for toxins in the pathogenesis and diagnosis of C. difficile infection. In a study investigating the natural history and need for treatment based on PCR and toxin enzyme immunoassay results, CDI-related complications and deaths occurred only in toxin-positive patients.16 Toxin-positive patients are also known to have more severe outcomes than toxin-negative CDI patients, and toxin-negative/PCR-positive patients have outcomes comparable to patients without C. difficile.16,17
Another study demonstrated that there was no difference in positivity rate between CDI suspects and asymptomatic inpatients when tested with PCR, suggesting that the majority of PCR-positive results among symptomatic patients are due to C. difficile colonization.18
Given what is known about the frequency of C. difficile colonization and the lack of correlation between nucleic acid amplification test results and C. difficile infection, the recommendation by IDSA/SHEA for standalone nucleic acid amplification testing among certain patient groups results in overdiagnosis of C. difficile infection.16–18
Future Options for CDI Diagnostics
The automated, rapid, in vitro diagnostic Singulex Clarity system, powered by single molecule counting technology, is able to detect analytes down to picogram-per-milliliter levels (see “Single Molecule Counting Technology“). The technology has been on the life science market for more than ten years and is backed by more than 180 peer-reviewed publications. The Clarity system and a cardiac troponin I assay are CE marked in the European Union.

Figure 5. The laser and detection vessel rotate on an x-y axis, and 150,000 data points are collected. The single molecule counting technology provides a reading range of up to six logs.
Singulex is now developing an ultrasensitive C. difficile toxin assay—the Singulex Clarity C. diff toxins A/B assay—with limits of detection at 0.8 and 0.3 pg/mL for toxin A and B, respectively—orders of magnitude lower than current commercially available toxin assays.19 Preliminary performance of the assay was presented at recent meetings of the European Congress of Clinical Microbiology and Infectious Diseases (ECCMID) and the American Society for Microbiology.
One of the ECCMID presentations showed that the Clarity toxin assay detected nearly all of the samples deemed positive by cell cytotoxicity neutralization assay (97.7%). The assay also detected toxins in 23% of samples deemed positive by PCR-based testing but negative by cell cytotoxicity neutralization assay, indicating that the Clarity assay can refine the selection of patients needing treatment.20
Another presentation comparing the Clarity toxin assay to a cell cytotoxicity neutralization assay found that the Clarity assay outperformed toxin enzyme immunoassays, PCR-based tests, and two multistep algorithms in terms of sensitivity and specificity. The researchers concluded that the assay offers ultrasensitivity and specificity in a single test, obviating the need for multistep algorithms, and potentially offering a standalone solution for the diagnosis of C. difficile infection.21
Solving the Conundrum
The diagnosis of C. difficile infection has been described as a “conundrum for clinicians and for clinical laboratories.”5 The need for less-complex testing strategies with better sensitivity, specificity, and turnaround times may soon be met. With an assay having both the sensitivity of nucleic acid amplification tests, and the innate specificity of toxin detection, future C. difficile diagnostic needs may be replaced with a single test. The Singulex Clarity C. diff toxins A/B assay has the potential to solve the conundrum and bring more certainty to the diagnosis of C. difficile infection.
Johanna Sandlund, MD, PhD, is a board-certified clinical microbiologist and associate director for clinical research at Singulex. For further information, contact CLP chief editor Steve Halasey via [email protected].
Featured Image: In 2016, the organism formerly known as Clostridium difficile underwent an official name change to become Clostridiodes difficile, acknowledging differences among the bacteria formerly grouped under the genus Clostridium. Medical illustration courtesy US Centers for Disease Control and Prevention.
References
- Magill SS, Edwards JR, Bamberg W, et al. Multistate point-prevalence survey of healthcare-associated infections. N Engl J Med. 2014;370(13):1198–1208; doi: 10.1056/nejmoa1306801.
- McDonald LC, Coignard B, Dubberke E, et al. Recommendations for surveillance of Clostridium difficile-associated disease. Infect Control Hosp Epidemiol. 2007;28(2):140–145; doi: 10.1086/511798.
- Crobach MJT, Planche T, Eckert C, et al. European Society of Clinical Microbiology and Infectious Diseases: update of the diagnostic guidance document for Clostridium difficile infection. Clin Microbiol Infect. 2016;22(Suppl 4):S63–S81; doi: 10.1016/j.cmi.2016.03.010.
- Hall IC, O’Toole E. Intestinal flora in newborn infants, with a description of a new pathogenic anaerobe Bacillus difficilis. Am J Dis Child. 1935;49(2):390–402; doi: 10.1001/archpedi.1935.01970020105010.
- Burnham CA, Carroll KC. Diagnosis of Clostridium difficile infection: an ongoing conundrum for clinicians and for clinical laboratories. Clin Microbiol Rev. 2013;26(3):604–630; doi: 10.1128/cmr.00016-13.
- Durham DP, Olsen MA, Dubberke ER, Galvani AP, Townsend JP. Quantifying transmission of Clostridium difficile within and outside healthcare settings. Emerg Infect Dis. 2016;22(4):608–616; doi: 10.3201/eid2204.150455.
- Di Bella S, Ascenzi P, Siarakas S, Petrosillo N, di Masi A. Clostridium difficile toxins A and B: insights into pathogenic properties and extraintestinal effects. Toxins. 2016;8(5):E134; doi: 10.3390/toxins8050134.
- Gerding DN, Johnson S, Rupnik M, Aktories K. Clostridium difficile binary toxin CDT: mechanism, epidemiology, and potential clinical importance. Gut Microbes. 2014;5(1):15–27; doi: 10.4161/gmic.26854.
- McDonald LC, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis. 2018;66(7):e1–e48; doi: 10.1093/cid/cix1085.
- Lessa FC, Mu Y, Bamberg WM, et al. Burden of Clostridium difficile infection in the United States. N Engl J Med. 2015;372(9):825–834; doi: 10.1056/nejmoa1408913.
- Pollock NR. Ultrasensitive detection and quantification of toxins for optimized diagnosis of Clostridium difficile infection. J Clin Microbiol. 2016;54(2):259–264; doi: 10.1128/jcm.02419-15.
- Tenover FC, Novak-Weekley S, Woods CW, et al. Impact of strain type on detection of toxigenic Clostridium difficile: comparison of molecular diagnostic and enzyme immunoassay approaches. J Clin Microbiol. 2010;48(10):3719–3724; doi: 10.1128/jcm.00427-10.
- Wilson V, Cheek L, Satta G, et al. Predictors of death after Clostridium difficile infection: a report on 128 strain?typed cases from a teaching hospital in the United Kingdom. Clin Infect Dis. 2010;50(12):e77–e81; doi: 10.1086/653012.
- Senchyna F, Gaur RL, Gombar S, Truong CY, Schroeder LF, Banaei N. Clostridium difficile PCR cycle threshold predicts free toxin. J Clin Microbiol. 2017;55(9):2651–2660; doi: 10.1128/jcm.00563-17.
- Kociolek LK, Gerding DN. Clinical utility of laboratory detection of Clostridium difficile strain BI/NAP1/027. J Clin Microbiol. 2016;54(1):19–24; doi: 10.1128/jcm.02340-15.
- Polage CR, Gyorke CE, Kennedy MA, et al. Overdiagnosis of Clostridium difficile infection in the molecular test era. JAMA Intern Med. 2015;175(11):1792–1801; doi: 10.1001/jamainternmed.2015.4114.
- Planche TD, Davies KA, Coen PG, et al. Differences in outcome according to Clostridium difficile testing method: a prospective multicenter diagnostic validation study of C. difficile infection. Lancet Infect Dis. 2013;13(11):936–945; doi: 10.1016/s1473-3099(13)70200-7.
- Truong C, Schroeder LF, Gaur R, et al. Clostridium difficile rates in asymptomatic and symptomatic hospitalized patients using nucleic acid testing. Diagn Microbiol Infect Dis. 2017;87(4):365–370; doi: 10.1016/j.diagmicrobio.2016.12.014.
- Bartolome A, Almazan A, Abusali S, et al. Evaluation of the Singulex Clarity C. diff toxins A/B assay, currently in development, for ultrasensitive detection of Clostridium difficile toxins [abstract P2282, online]. Presentation at the annual meeting of the European Congress of Clinical Microbiology and Infectious Diseases, Madrid, April 21–24, 2018. Available at: www.escmid.org/escmid_publications/escmid_elibrary. Accessed July 25, 2018.
- Sandlund J, Bartolome A, Bishop J, et al. Clinical evaluation of the Singulex Clarity C. diff toxins A/B assay, currently in development, for ultrasensitive detection of Clostridium difficile toxins A and B [abstract P2281, online]. Presentation at the annual meeting of the European Congress of Clinical Microbiology and Infectious Diseases, Madrid, April 21–24, 2018. Available at: www.escmid.org/escmid_publications/escmid_elibrary. Accessed July 25, 2018.
- Bartolome A, Almazan A, Abusali S, et al. Preliminary performance evaluation of an automated Singulex Clarity C. diff toxins A/B assay and comparison to PCR and multistep algorithms [abstract P2283, online]. Presentation at the annual meeting of the European Congress of Clinical Microbiology and Infectious Diseases, Madrid, April 21–24, 2018. Available at: www.escmid.org/escmid_publications/escmid_elibrary. Accessed July 25, 2018.



{kind=link}