The Implications for Histotechnologists’ Job Security
By Gary Tufel
The field of histotechnology encompasses a variety of technical processes that enable anatomic pathologists to review slides of patient samples in order to develop a diagnosis. In recent years, traditional histological visualization has been supplemented by digital pathology applications that make use of advanced staining and imaging technologies. Such advances are offering new opportunities for histotechnologists to be on the cutting edge of clinical diagnosis as well as patient management.
Digital pathology has focused primarily on whole-slide imaging (WSI), in large measure because of its potential for instantaneous sharing of images with consulting pathologists. The realization that histology may also benefit from the use of digital pathology is more recent.
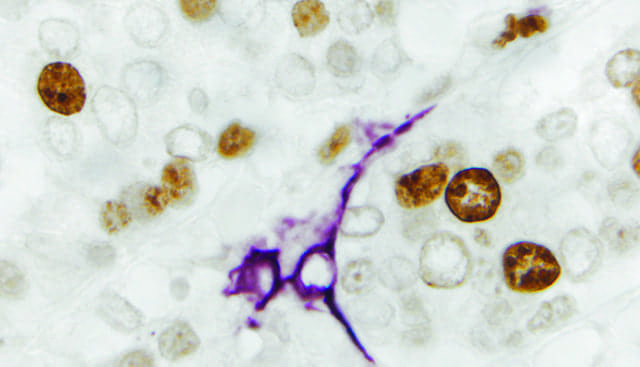
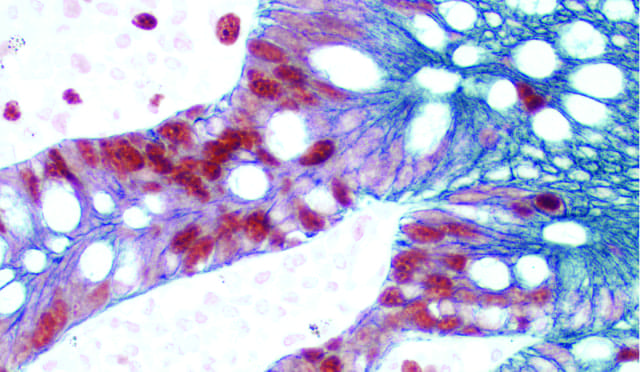
Breast carcinoma: Ki67 (rm), ImPRESS reagent (HRP; universal), Vector DAB (brown); CD34, ImmPRESS reagent (HRP; universal), Vector VIP (purple).
Some experts anticipate the emergence of a new type of specialist, the “imaging technologist,” whose responsibilities include overseeing all aspects of the digital pathology workflow, and partnering with pathologists to improve their practice and deliver on the promise of electronic healthcare.
The rise of imaging technologists represents an extension of the same attention to detail that histotechnologists have always had, but now with advanced tools to help quantitate and monitor their observations. When used in approved diagnostic applications, for instance, digital pathology scans rely on quality control (QC) processes to ensure that the correct diagnosis is made. Imaging technologists will be expected to anticipate and address quality-related concerns such as whether the stain colors remain true after digitization, whether an entire tissue sample was scanned, or whether there are issues with a scan’s focus.
When dealing with slides that will be scanned, histotechnologists will have to adapt to this new digital world by adhering to policies and procedures that define proper tissue orientation, thickness, staining, and other qualities. In the past, pathologists have generally been forgiving of such histotechnologist slide-mounting miscues as a small fold or tear, or differences in staining intensity. But in the future, they will tend to be much more critical of whole-slide imaging scans of poorly sectioned or stained tissues. The digitization process magnifies errors, say the experts.
Whole-slide imaging can also be used to help with QC for staining, by tracking changes in stains over time. The same rigor as that applied to tests in a clinical chemistry laboratory can now be applied to histology slides. The development of new immunohistochemistry (IHC) stains will benefit from the digitization of slides having different antibody titers. Through the adoption of digital pathology, say the experts, histology will end up adopting the same rules and guidelines as those common in clinical lab QC charting.
REPEATING THE REVOLUTION

William DeSalvo, BS, HTL(ASCP), Sonora Quest Laboratories.
“In my mind, the most difficult challenges involving histotechnology and the adoption of digital pathology are those related to standardization, or the lack thereof,” says William DeSalvo, BS, HTL(ASCP), system production manager for anatomic pathology at Sonora Quest Laboratories, Phoenix. “The entire process of anatomic pathology testing suffers because it is dominated by open procedures and open instrumentation that offer too many ways of performing the same task. There’s too much subjective decision-making, with too little control of the processes.”
Symptomatic of such subjectivity, says DeSalvo, process variations contribute to the sorts of diagnostic discordance detected in a recent study of pathologists’ interpretations of breast biopsy slides, which suggested that nearly 25% of such decisions might be in error.1,2 “Variations in manual staining, and difficulties in implementing digital pathology and whole-slide imaging, are magnifying variation issues, from pathologist to pathologist and particularly from lab to lab,” says DeSalvo. He adds that labs spend a great deal of time performing archaic quality control activities, when that time could be better spent on quality assurance.
Federal government support for programs in precision and personalized medicine—including the use of targeted therapies—has also brought renewed attention to the field of histotechnology. Although most of the activity in this area is currently concentrated on the development of targeted biopharmaceuticals, a central role is being played by the labs and pathologists who prepare and supply tissue samples to oncologists for diagnosis. “But the methods they are using are more than a hundred years old,” says DeSalvo. “Manually collecting, processing, and staining slides for analysis is both time-consuming and subject to variation. And even semiautomated methods of processing tissues for analysis are associated with a significant lack of standardization.”

A tray of patient slides to be stained individually with fresh reagent on a fully automated staining system.
Recognition of the need for faster and more-standardized tissue processing has recently led to an increase in laboratory adoption of automated histotechnology systems. But with its advantages, automation also offers some significant challenges, one of which is the continuing dearth of comparable automation across the laboratory sector. Many laboratorians and others hope for a repeat of the revolution that took place in many clinical chemistry labs 25 years ago, bringing about full automation and standardization in a single swoop.
MANUAL VERSUS AUTOMATION
Despite the introduction of growing numbers of automated histotechnology products, a significant number of labs still use manual methods of staining and processing slide samples. Such manually stained tissue samples are almost impossible for another lab to reproduce, and thus inhibit interoperability and result in quality issues.
A rack of patient slides is transferred from one stain vessel to another.
With standardization, histotechnology results are controllable and can be correlated to one another across a manufacturer’s systems and the labs that use them. A drawback of this approach is the fact that such standardized systems are closed—requiring use of the manufacturer’s proprietary technologies at every step—unlike manual systems that can utilize reagents and other technologies from a variety of manufacturers.

Beth Sheppard, MBA, HT(ASCP), National Society for Histotechnology.
Histotechnology is likely to be one of the last areas in the clinical laboratory to become fully automated, strictly due to the need for human intervention in some of its basic processes, such as paraffin embedding and tissue block cutting, says Beth Sheppard, MBA, HT(ASCP), president of the National Society for Histotechnology.
“Automation provides a standardized process that ensures accurate, reproducible results. However, automation also creates opportunities, since instrumentation only works as well as the operator,” says Sheppard. “Even when the process is automated, the technologist still needs to understand the process, know how to troubleshoot it, be able to employ alternative solutions, and have a grasp on good quality control. The technologist has to understand how to determine whether the results are reliable. Only a well-trained histotechnologist can employ these valuable tools.
“There are many prospects for the histotechnologist today, mostly because of the advanced testing of tumors and other tissues to help make very important decisions that can facilitate savings downstream by directed therapy,” adds Sheppard. “They are the facilitators of upstream tissue standardization that is needed to produce reliable results and understand the importance of a good diagnostic slide.”

Angie Cahill, MBA, HT(ASCP), Ventana Medical Systems.
In medical laboratories, the prevalence and scope of automation is continuing to grow every year, says Angie Cahill, MBA, HT(ASCP), senior international product manager at Ventana Medical Systems Inc, Tucson, a member of the Roche Group. But the level of mechanization varies widely among various laboratory departments.
“A blood sample collected from a patient and introduced to a fully-automated clinical core lab system may never again be touched by a human. It can be automatically centrifuged, aliquoted, sorted, routed, tested, reintroduced later for additional ordered tests, and even discarded at the end of its usable life,” notes Cahill “This streamlined process is contrasted by the processes used in the histology laboratory, where sample-handling automation has made progress—but not to the same extent. Solutions exist in the histology market to automate some processes, but not in a seamless fashion that encompasses the entire workflow. Many histology labs still rely heavily on manual steps performed by technicians.”
Tissue staining is one area in which tremendous progress toward automation has been made in recent decades. Options are readily available for labs to automate hematoxylin and eosin (H&E) staining, IHC staining, in situ hybridization (ISH) staining, and special stains. However, some labs still choose to stain manually or in a semiautomated manner.
A technologist transfers a rack of patient slides from one stain vessel to another.
Many labs still use manual procedures for H&E staining. In this process, a technician prepares the reagents, transfers groups of patient slides from one reagent vessel to another in a linear fashion, and then coverslips the slides by hand, one at a time. The cost of the supplies needed to perform such manual processes is relatively inexpensive, but the workflow and labor components of executing all of a lab’s staining by hand should also be considered, as they can raise costs significantly.
Even semiautomated staining processes can run afoul of challenges. “Traditional, linear H&E stainers eliminate the need for operators to manually move slides from vessel to vessel, but they do not remove the quality and safety challenges associated with the process,” says Cahill. “Quality and consistency challenges result from reagent and tissue-floater carryover from staining vessel to staining vessel. Open reagent baths lead to oxidation and precipitation, degrading reagent integrity. And with both manual staining and semiautomated linear strainers, there is also a risk of technician exposure to potentially harmful reagents.”
A number of manufacturers now offer fully prepared reagents, helping to advance gains in histology quality, workflow, and safety. The integration of ovens and coverslippers with semiautomated stainers has also proven to be a strong step toward improving H&E staining workflow. But neither of these improvements has succeeded in eliminating the challenges of variability in quality and patient safety.
“The advent of H&E staining systems that not only integrate and automate these additional tasks, but also stain each patient slide individually with fresh, ready-to-use reagents, has ushered in a new era of improved workflow and quality, while mitigating issues with patient and technician safety in H&E staining,” says Cahill. “In the future, the automation progress already realized in tissue staining, in combination with other preanalytic automation technologies, could produce a fully-automated histology laboratory.”
TRANSFORMATIVE CHANGES
For Mansoor Nasim, MBBS, MD, PhD, FCAP, assistant professor of pathology and laboratory medicine at Hofstra North Shore LIJ School of Medicine, and vice chair of the histotechnology committee of the College of American Pathologists (CAP), a key issue is how histotechnologists will survive the uncertainties of the coming healthcare environment, when hospitals are unsure of their revenue channels. (For more information, see the companion article, “The New-Model Histotechnologist.”)

Currently under development, the Ventana HE 600 system is a fully automated H&E staining solution with individual slide staining technology to virtually eliminate the risk of tissue cross contamination.
The creation of accountable care organizations has been heralded as the pathway toward eliminating fee-for-service medicine, and achieving a better alignment between healthcare payers and providers. But so far, it isn’t clear that such realigned incentives have succeeded in convincing physicians to take on new approaches to patient care—including advanced diagnostic technologies. In fact, the new organizations are intentionally designed to incentivize physicians to do less rather than more—including less diagnostic testing. In such a changed environment, Nasim wonders, how will reimbursement for a simple H&E stained slide be able to survive the rigors of the new payment plan?3,4
To navigate the pitfalls of the emerging healthcare environment, says Nasim, it will be necessary for histopathologists to seek out new avenues of revenue. “We need anatomic pathology to be associated with the technologies used in molecular pathology,” he says. “Already, chromogenic in situ hybridization (CISH) staining is revolutionizing the way we perform testing for HER2 genetic mutations. And in the future, the use of CISH will become common in diagnostic testing for such viruses as herpes simplex virus and cytomegalovirus, as well as in the testing of paraffin-embedded gliomas for loss of heterozygosity on chromosomes 1p and 19q.5 Many don’t realize it, but histotechnology is already in molecular mode.”
“Already transformative changes have started, as in radiology,” Nasim notes. “Are these changes going to happen in anatomic pathology? Digital slide implementation is certainly in the future, but the question is when, and what effects will it have?”

Craig Pow, PhD, Vector Laboratories.
For the foreseeable future, at least, histotechnology will remain a mainstay of clinical laboratories. “Histotechnology has evolved from humble manual applications to high-throughput automated systems, and from single staining to multiple staining on the same section. Additionally, tedious routine slide reading by pathologists is shifting to more digital approaches, using imaging software capabilities with sophisticated algorithms,” says Craig Pow, PhD, director of business development and international marketing for Vector Laboratories, Burlingame, Calif.
“Nevertheless, the basic goal of identifying expressed antigens of interest remains the same. How that information is collected and evaluated will continue to take shape. Some companies offer systems that enable the placement of slides on a microscope that is linked via the Internet to a consulting pathologist elsewhere in the country. The system enables the lab that submitted the sample to speak with the consulting pathologist about his observations in real time,” Pow notes.
Nasim foresees the development of anatomic pathology training programs that encompass laser microdissection, histopathology, DNA and RNA procurement for tissue, and information technologies—all integrated with the use of second-generation sequencing equipment. In conjunction with such new programs, he suggests, there will be a need for better use of information technologies—both in programs for teaching and in candidate recruitment.
“There are critics who oppose creating such programs,” says Nasim, “but the choice is between having histotechnologists remain low-salaried or enabling the profession to become the master of its own destiny. The profession cannot attract quality techs without a quality pay structure,” he adds.
CONCERNS ABOUT AUTOMATION
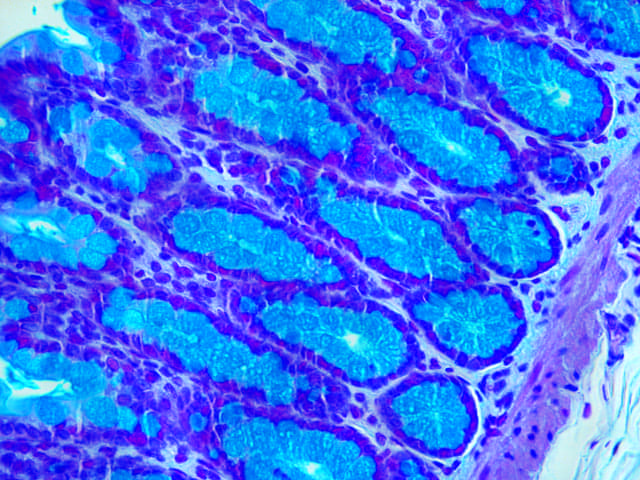
Small bowel: Ki67 (rp), ImmPRESS reagant (HRP; universal), Vector NovaRED (red); cytokeratin 8/18 (m), ImmPRESS reagent (HRP; universal), Vector SG (blue-gray).
As might be imagined, automation helps to alleviate the staff shortages that are often found in clinical laboratories. “The implementation of automated systems provides laboratories with needed efficiencies and the ability to add to the advancing diagnostic test menu,” says NSH’s Sheppard. But it also results in “a reallocation of technologists to areas that are less automated.”
“Technicians are not replaced by automation,” agrees Cahill. “Automation replaces unfilled positions and enables staff to use their highly specialized training and skills to continuously improve how the lab runs—not just to struggle toward completing the daily workload.”
Nevertheless, in all parts of the lab, concern has long existed about the effects of increased automation on the job security of medical technologists. “Whenever laboratories were evaluating new technologies, the fear that automation would replace technicians was palpable. Over the years, however, something very different proved true,” says Cahill. “A chronic lack of qualified technicians drove lab management to find alternate ways to complete the workload when open positions went unfilled. This is still happening today, and it is expected to become even more challenging with a generation of histotechnicians nearing retirement and insufficient numbers of newly minted technicians to take their place. Manufacturers have responded to the call from lab management for expanded automation options.”
Automated equipment is a must, agrees Nasim. And there is an especially strong need for new instruments that can embed, cut, and stain tissue samples. “Already, new automated H&E stainers are in vogue, and cutting platforms are springing up.
“New automated immunohistochemistry platforms by Dako, Leica, and Roche are becoming the standard and leading the way,” Nasim adds. “Previously, preparing an immunostain would have taken at least 2 working days. Now, with better antibodies, turnaround time can be as little as a few hours, depending on the antibody stain. Already, this technology is cutting costs, reducing processing time, increasing the number of cases being done, and resulting in the hiring of more specialized trained personnel.”
Gary Tufel is a contributing writer for CLP. For further information, contact CLP chief editor Steve Halasey via [email protected].
REFERENCES
- Elmore JG, Longton GM, Carney PA, Geller BM, et al. Diagnostic concordance among pathologists interpreting breast biopsy specimens. JAMA. 2015;313(11):1122–1132; doi: 10.1001/jama.2015.1405.
- Kaplan KJ. More thoughts on JAMA breast biopsy study. Digital Pathology Blog. May 12, 2015. Available at: http://tissuepathology.com/2015/05/12/more-thoughts-on-jama-breast-biopsy-study/#ixzz3gj3vfiST. Accessed August 1, 2015.
- Johnson C. A revolution in how doctors are paid isn’t really changing how doctors are paid. Washington Post. July 20, 2105. Available at: http://www.washingtonpost.com/news/wonkblog/wp/2015/07/20/the-health-care-revolution-to-change-how-doctors-are-paid-that-isnt-actually-changing-how-doctors-are-paid. Accessed August 1, 2015.
- Ryan AM, Shortell SM, Ramsay PP, Casalino LP. Salary and quality compensation for physician practices participating in accountable care organizations. Ann Fam Med. 2015;13(4):321–324; doi: 10.1370/afm.1805.
- Lass U, Hartmann C, Capper D, et al. Chromogenic in situ hybridization is a reliable alternative to fluorescence in situ hybridization for diagnostic testing of 1p and 19q loss in paraffin-embedded gliomas. Brain Pathol. 2013;23(3):311–318; doi: 10.1111/bpa.12003.



{kind=link}