
Artificial intelligence is reshaping the capabilities and practices of modern pathology laboratories
By David West Jr
For the past 150 years, pathologists have made diagnoses by looking at tissue specimens under a microscope. Today, digital whole-slide imaging (WSI) allows the capture and visualization of the entire tissue on a slide, as opposed to the narrow field of view that a microscope provides. The image files that are produced from whole-slide imaging systems are very large and are usually scanned at a magnification of 20x or 40x. This enables pathologists to capture a great deal of detail that was not previously visible (see Figure 1).
Yet, capturing the image is just the start of a process that promises to transform pathology. Once in the ‘digital realm,’ where pathologists are dealing with pixels rather than glass, two key benefits arise:

Figure 1. Digital whole-slide imaging (WSI) allows the capture and visualization of the entire tissue on a slide, as opposed to the narrow field of view that a microscope provides. Files produced by WSI systems are very large and are usually scanned at a magnification of 20x or 40x, enabling pathologists to capture a great deal of detail that was not previously visible.
Distance no longer matters. Sending slides between institutions on different sides of the world becomes much easier, opening up new possibilities for collaboration, helping pathology departments and private labs to grow, and improving access to subspecialty experts—especially for patients in remote areas. No longer does a consultation have to wait on physical tissue, with all the expense and regulation involved in sending biological materials.
Computational pathology brings precision capabilities to anatomic pathology. Image analysis algorithms can operate on the images, leveraging data provided by the pixels. Such algorithms are already being used for automated or semiautomated immunohistochemistry (IHC) quantification, helping to drive standardization and speed of analysis, and new methods are under development to augment hematoxylin and eosin (H&E) staining analyses. The application of image analysis algorithms could play a profound role in reducing interobserver variability for many diagnoses, and drive faster, more-precise quantification of the essential elements of existing pathology workflows.
The application of machine learning and artificial intelligence to digital pathology promises to reshape the capabilities and practices of modern pathology laboratories.
Current Challenges in the Pathology Lab
From a broad perspective, digital pathology offers an opportunity to address many of the biggest challenges facing pathology labs today. These include the following.

Figure 2. There is a global shortage of pathology expertise. The ratio of patients per pathologist is extremely high in many areas of the world. Digital pathology offers an opportunity to make expertise more available to remote areas.1–2, 7, 14–18
A shortage of pathologists. The number of pathologists is predicted to decrease, both in the United States and globally. There are some parts of Africa that have one pathologist for every 1.5 million people.1 In the United States, practicing pathologists will begin to retire at an increasing rate, peaking in 2021, far faster than the current replacement rate.2 And all of this is taking place at a time when there are an increasing number of cases and data that require pathology attention, leading to pathologists taking on more cases than ever before (see Figure 2).
Lack of subspecialty expertise. The challenge of decreasing numbers of pathologists does not stop with caseloads. If the required subspecialty expertise is not available onsite, those very specific and challenging cases must be sent elsewhere. It is expensive and time-consuming to send a physical glass slide across the country, or even out of the country.
 Problems with accuracy and reproducibility. Despite its scientific underpinnings, anatomic pathology is fraught with subjectivity; for example, pathologists often make manual estimates of the percentage of positive calls for a particular biomarker. Studies have shown that for some cancers, pathologists analyzing tissue agree on a diagnosis only 55% of the time.3 Access to technologies that augment the work of a pathologist by providing more accurate and reproducible analysis of key factors will improve patient outcomes, especially in the diagnosis of extremely complex and variable diseases such as cancer (see Table 1).
Problems with accuracy and reproducibility. Despite its scientific underpinnings, anatomic pathology is fraught with subjectivity; for example, pathologists often make manual estimates of the percentage of positive calls for a particular biomarker. Studies have shown that for some cancers, pathologists analyzing tissue agree on a diagnosis only 55% of the time.3 Access to technologies that augment the work of a pathologist by providing more accurate and reproducible analysis of key factors will improve patient outcomes, especially in the diagnosis of extremely complex and variable diseases such as cancer (see Table 1).
Focus on reducing costs and increasing efficiencies. Healthcare providers everywhere are under pressure to control costs, and pathology labs are no different. In most hospitals and academic medical centers, a pathology laboratory is considered to be a cost center.4 Depending on the setting, labs may have the potential to make money by handling outside consultations, but most of the time this is not the case. Moreover, most pathology labs are not effectively integrated with the clinical operations of their companion hospitals and medical centers. With many other aspects of healthcare moving to a digital workflow—such as electronic medical records (EMRs), radiological imaging, and so on—it would make sense for pathology labs to do the same. One of the main drivers behind healthcare costs is the inefficiency of diagnosis and testing.5
The ROI of Digital Pathology Today
Technical merit is necessary but not sufficient for the adoption of a transformative technology. In addition to technical performance, a new technology must demonstrate a clear and definite savings in time or money, or an improvement in the effectiveness of services provided. Ideally, it should demonstrate success in all three.
Digital pathology is rightfully gaining attention among pathology labs because it offers a clear return on investment (ROI). The most obvious and immediate impact is on workflow. Digital pathology has been shown to improve the efficiency of pathology workloads by 13%.6 Simply moving from examining tissues under a microscope to using a monitor offers a clear cost advantage by improving the workflow of the laboratory. Digital pathology can also address many other direct costs, including the following.
Quantitative assessment and international consultations. Some of the most costly ventures encountered by every lab involve providing consultations and quantitative IHC assessments. On average, a lab charges anywhere from $200 to $300 per consultation. Today, labs can exponentially grow these revenue streams with digital pathology software.
International consultations are important, especially for patients in remote areas of countries such as China, where subspecialty expertise is sparse compared to the number of cases. In China, the number of pathologists per capita is just one-fourth of the equivalent number in the United States. Effectively, this means that each Chinese pathologist must see four times the number of cases in order for patients to be provided the same level of pathology services as found in the United States.7
With digital pathology, international consultations are as simple as uploading the tissue image into the Cloud, giving pathologists the ability to analyze the tissue within the day rather than wait weeks for the physical tissue to arrive.
Digital pathology can also increase lab revenue by automating quantitative IHC assessments. For labs that adopt digital pathology technologies, this means that reimbursement can be increased by using CPT codes 88360 and 88361 for semi quantitative and quantitative IHC. Automation of these processes does not affect reimbursement, but can affect the efficiency of performing these services, thereby lowering the lab’s costs and making the lab a more attractive source for performing such tests on a consulting basis.
Consolidation and courier replacement. Many pathology departments have a central histology lab that prepares tissues and makes slides. The tissue and resulting slide are shipped back and forth between the surgeon who took the tissue, the lab, and the pathologist through a courier service specializing in transporting tissue. In some circumstances, the lab may be located hours away from the doctors. All this takes time, and it is expensive. Digitizing a slide eliminates the need to ship to remote locations.
Control slides. Currently, when histology labs receive multiple requests for specialty slides to be prepared and stained in the same manner, a control slide must also be made for each case. Control slides do not use patient tissue, but are made with lab cell cultures prepared with the same stains as the patient tissue and used as reference to a known positive or known negative. Although the cost of a single control slide may seem insignificant—approximately $8 to $12, depending on the case and institution—a large operation may make hundreds of control slides each day. In an industry where margins matter, these costs add up.
With digital pathology scanners and software, labs only need to produce one control slide per stained batch instead of one control slide per stain per pathologist. Histology labs then scan this single control slide and make that digital image available to all pathologists who are inspecting tissues from that batch. This streamlined process reduces the number of control slides considerably, and also reduces or eliminates the costs associated with the couriers once needed to ship the slides to each pathologist. The Cleveland Clinic was able to save on the order of $30,000 to $50,000 in 6 months just by cutting down on its creation of control slides.8
A further advantage to reducing the creation of control slides and minimizing the use of couriers is that both changes can be applied to clinical medicine without triggering the need for FDA approval.
Better specimen tracking. Before slides are made, the specimen needs to be delivered to appropriate labs and physicians. Although the use of bar coding has increased accountability and reduced errors in the lab, specimen tracking remains a very complicated process, and technicians and pathologists can still have issues during manual case assembly, leaving opportunities for mishandling the specimen. With a digital pathology system, case assembly and transportation to a pathologist is fully automated, eliminating human error in the handling of slides.
Reduced breakage. By sending the resulting slide to the ordering pathologist in the form of a digital image, digital pathology also reduces the likelihood of slide breakage or loss in transit. Pathologists who are relaying digital slides are not transmitting fragile pieces of glass. The slide is able to remain stationary in a digital archive and, therefore, the chances of breakage are eliminated.
Finally, there is one soft cost saving that many pathology labs are finding compelling: the elimination of distance as a factor in collaboration and consultation. In the past, collaboration was a slow and often expensive process, requiring the shipment of individual slides to experts in remote locations. Response time was often measured in weeks, especially if a slide needed to be sent to another country. Digital pathology removes those barriers. It is now simple to send images to any location, and multiple people can consult on the same image simultaneously.
The Rise of Computational Pathology
Once a slide image is in the digital realm, it becomes possible to apply machine learning and artificial intelligence techniques to the digital pathology images. It is vastly easier to move and manipulate bits of information than it is the atoms and molecules of physical tissue. The economics of the computer industry now apply. Calculations that used to be exorbitantly expensive to perform cost only pennies a few years later.

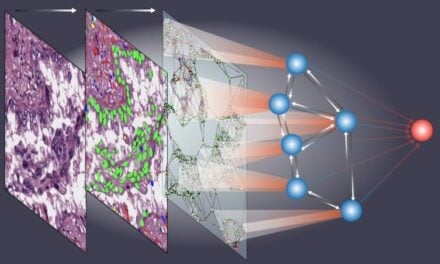
Figure 3. Computational pathology involves applying machine learning and artificial intelligence techniques in a multi-layered process to perform image analysis, quantification, and classification.11
‘Computational pathology’ is a term that’s starting to become more common in the pathology field as computer processing power is being applied to managing, analyzing, and interpreting slide images (see Figure 3). There are three main elements that make up computational pathology: automation, augmentation, and prediction.
Automation. Automation involves computer-assisted software helping to speed up workflow and making it easier for a pathologist to work with slide images. This concept is not new, and there are already many precedents for the adoption of automation in pathology. Pathologists have been creating automated solutions for Pap smears and cervical cancer screening since the 1960s.9

Figure 4. Preprocessing of whole slide images enables automated image recognition systems to interpret images more effectively and more accurately. Shown here are five transformations (a-e) compared against the original image (f). The white contour (f) highlights areas of tissue and reduces the number of pixels the system needs to process.11
Yet the bulk of practitioners in the field of pathology are just now starting to catch up with regard to automation, especially as it pertains to highlighting areas of a tumor. But it can save a lot of time and effort if a pathologist can utilize software that prescreens slides. Much of what a pathologist looks at is benign, with the exact breakdown of benign versus malignant varying by cancer type.10 Automated image recognition systems that identify slides with precancerous or cancerous cells enable pathologists to spend more of their time on the slides whose diagnosis requires greater attention (see Figure 4).
Automation could help address the shortage of pathologists by removing clearly benign slides from the workflow. According to one study, by 2030 the number of active pathologists may decrease by approximately 30% compared to 2010 levels.2 With automation, patients will not have to wait longer for a diagnosis, despite the decreasing number of practitioners in the pathology workforce.
Augmentation and Precision. Augmentation goes a step beyond automation, enabling pathologists to identify abnormalities in tissue that the human eye couldn’t otherwise see, even with a microscope. Similar to automation, augmentation is nothing new to the pathologist. Molecular tests are commonly used to illuminate a protein that a pathologist never would be able to view because it is transparent in color, and the human eye could not detect it unless the tissue is stained with a chemical that binds to that particular protein.
But with the amazing strides that technology has taken in the past 20 years, augmentation of digital pathology images is entering a new era of precision medicine. For example, augmentation could integrate computer-quantified histology data from a slide with data from other sources, such as DNA sequencing, helping pathologists to draw conclusions with greater accuracy and confidence.
Another use of augmentation is counting and differentiating cell types to help with the staging of tumors. Pathologists often rely on visual estimates to perform staging, introducing a level of subjectivity. Augmentation that automatically counts cell types enhances standardization and reproducibility.
Quantitative IHC is an existing technology that is already in widespread use. In fact, Proscia offers its own branded quantitative IHC algorithms, labeled for research use only. Pathologists can also do this task themselves, but quantitative IHC does it more quickly and more accurately—and the algorithm will provide the same result every time.
In the same sense that certain molecular tests are able to provide more information, image-based diagnostic tests can also provide more information and should be appropriately reimbursable. This may spur some far-sighted laboratories to use computational pathology to provide laboratory-developed tests as a new and powerful service for their existing clients. A key distinguishing factor between digital pathology and other transformative technologies is that it integrates seamlessly into pathologists’ existing day-to-day work activities as another tool to be applied in their diagnoses.
Prediction. Prediction is the most important aspect of computational pathology. Advances in digital pathology have enabled the extraction of clinically relevant quantitative histology information, particularly from cancer tissue. The goal is to apply mathematical oncology and novel deep-learning approaches to provide predictive insight into the likelihood of metastasis, disease progression, and other clinically valuable predictions that improve a physician’s ability to prescribe targeted cancer therapies.
While there are currently no FDA-approved applications for image-based prognostics, important strides are being made in research laboratories. Proscia, for example, has demonstrated the ability to use quantitative histology to determine the likelihood of lymph node metastasis in breast cancer.11
Metastatic presence in lymph nodes is one of the most important prognostic variables of breast cancer. The current diagnostic procedure for manually reviewing sentinel lymph nodes, however, is very time-consuming and subjective. Pathologists have to manually scan an entire digital whole-slide image for regions of metastasis that are sometimes detectable only under high resolution, or are entirely hidden from the human eye. (For more information, see “Digital Pathology versus Radiology.”)
Using a generalizable stain normalization technique and a Cloud-based digital pathology platform, Proscia trained a deep convolutional neural network on millions of tissue and tumor image tiles to perform slide-based evaluation on a testing set of whole-slide images. The software was able to identify metastases with a sensitivity of 0.96, specificity of 0.89, and an AUC score of 0.90. The results indicated that the Cloud-based software could automatically scan any whole-slide image for metastatic regions without institutional calibration to respective stain profiles.
Conclusion
Every pathology lab should be planning to go digital. There are compelling use cases for digital pathology that provide a return on investment in the near term. The technology also provides the foundation for automation, augmentation, and predictive analysis, as advanced artificial intelligence techniques are applied to now-digitized whole-slide images.
Labs must put a scanner in place. The cost of scanners is beginning to fall, bringing them into line with the cost of the more-advanced microscopes in use at many pathology labs. Recent FDA approval of a digital pathology scanner for primary diagnoses in clinical applications shows that the technology is maturing quickly.12 Labs can expect that more scanners will be given FDA approval in the coming few years.
But even without FDA approval, labs can already take advantage of digital pathology for offering second opinion consultations. Other use cases for digital pathology (control slides, courier replacement, quantitative IHC) are either unregulated by FDA or already approved.
There is a growing shortage of pathologists—especially specialists—and digital pathology eliminates distance as a factor in building a consultative practice. With a scanner in place, a laboratory can begin taking advantage of digital pathology software, which offers benefits on both the cost and revenue side of the business:
- Digital pathology enables labs to control costs by working more efficiently.
- It also offers an opportunity to drive top-line revenue growth by expanding remote consultation.
Going digital is also essential for taking advantage of computational pathology. While the benefits of computational pathology are a few years away, the labs that build up their experience with digital tools and workflows will be best positioned to take advantage when the software becomes the laboratory.
David West Jr is CEO of Proscia Inc. For further information contact CLP chief editor Steve Halasey via [email protected].
References
- Park S, Parwani AV, Aller RD, et al. The history of pathology informatics: a global perspective. J Pathol Inform. 2013;4:7; doi: 10.4103/2153-3539.112689.
- Robboy SJ, Weintraub S, Horvath AE, et al. Pathologist workforce in the United States, I: development of a predictive model to examine factors influencing supply. Arch Pathol Lab Med. 2013;137(12):1723–1732; doi: 10.5858/arpa.2013-0200-OA.
- Wong AT, Agarwal M, Navo EB, et al. Concordance of Gleason score on biopsy and after prostatectomy: a SEER database analysis. J Clin Oncol. 2015;33(no. 7_suppl):50-50; doi: 10.1200/jco.2015.33.7_suppl.50.
- Ascending from the basement: hospital laboratories can become profit centers . San Antonio, Tex: Frost & Sullivan, 2012. Available at: http://www.frost.com/prod/servlet/cio/261240248. Accessed September 13, 2017.
- The human cost and financial impact of misdiagnosis [white paper, online]. Baltimore, Md: PinnacleCare, 2016. Available at: www.pinnaclecare.com/download/human-cost-financial-impact-whitepaper.pdf. Accessed September 13, 2017.
- Ho J, Ahlers SM, Stratman C, et al. Can digital pathology result in cost savings? a financial projection for digital pathology implementation at a large integrated health care organization. J Pathol Inform. 2014;5(1):33; doi: 10.4103/2153-3539.139714.
- Cornish T. Global insourcing using a pathology teleconsultation network platform [online]. Presented at Pathology Visions 2014 (San Francisco: 20–21 October 2014). Available at: https://digitalpathologyassociation.org/_data/files/2014_pathology_visions/pv14_presentations/19c_in-sourcing_workshop_cornish.pdf. Accessed September 12, 2017.
- Slaw RJ. Use cases and their after-effects: the scans that keep on giving [webinar, online]. Carmel, Ind: Digital Pathology Association, 2017. Available at: https://digitalpathologyassociation.org/2017-dpa-webinar-series-session-3. Accessed August 28, 2017.
- Bengtsson E, Malm P. Screening for cervical cancer using automated analysis of PAP-smears. Computational and Mathematical Methods in Medicine. 2014; article ID 842037, 12 pages; doi: 10.1155/2014/842037.
- Woodhouse JG, Tomecki KJ. Common benign growths [online]. Cleveland: Cleveland Clinic Foundation, 2017. Available at: www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/dermatology/common-benign-growths. Accessed September 11, 2017.
- Chen R, Jing Y, Jackson H. Identifying metastases in sentinel lymph nodes with deep convolutional neural networks [online]. Baltimore: Proscia, 2016. Available at: https://arxiv.org/pdf/1608.01658.pdf. Accessed September 11, 2017.
- FDA allows marketing of first whole slide imaging system for digital pathology [news release, online]. Silver Spring, Md: FDA, 2017. Available at: www.fda.gov/newsevents/newsroom/pressannouncements/ucm552742.htm. Accessed August 28, 2017.
- Saco A, Ramírez J, Rakislova N, Mira A, Ordi J. Validation of whole-slide imaging for histopathological diagnosis: current state. Pathobiology. 2016;83(2-3):89–98; doi: 10.1159/00044823.
- Graves D. Pathology’s workforce crisis: impact on acute healthcare in Australasia [online]. Global Healthcare Technology. Available at: www.healthtechglobal.com/knowledge-share/articles/pathologys-workforce-crisis-impact-on-acute-healthcare-in-australasia.php. Accessed September 13, 2017.
- Colgan TJ, Geldenhuys L. The practice of pathology in Canada: decreasing pathology supply and uncertain outcomes. Arch Pathol Lab Med. 2012;136(1):90–94; doi: 10.5858/arpa.2011-0188-OA.
- McBride M. Severe shortage of pathologists threatens Israel’s health system—especially cancer testing [online]. Dark Daily. Available at: http://www.darkdaily.com/severe-shortage-of-pathologists-threatens-israels-health-system-especially-cancer-testing-51711. Accessed September 13, 2017.
- Borracci R. Number of cardiologists in Argentina: report based on the Argentine integrated healthcare information system. Rev Argent Cardiol. 2014;82(4):308–311; doi: 10.7775/rac.v82.i4.3938.
- Report of the National Task Force on Medical Staffing. Dublin, Ireland: Republic of Ireland Department of Health, 2003. Available at: http://health.gov.ie/wp-content/uploads/2014/03/Report-of-the-National-Task-Force-on-Medical-Staffing-Hanly-report.pdf. Accessed September 13, 2017.



{kind=link}
Great Blog! Thanks for sharing the benefits of Digital Pathology.