
Blood and test utilization programs can improve patient care while reducing health system costs.
By Diane Janowiak and Tim Hannon, MD, MBA
In the realm of transfusion medicine, as in the healthcare sector as a whole, achieving high-value care is the goal of healthcare systems and providers who endeavor to improve patient results and reduce costs. Clinical laboratories can play an important role in this effort by helping to reduce or eliminate unnecessary testing and blood transfusions.
Lab testing is the single highest volume medical activity in a health system, with an estimated 4 billion to 5 billion tests performed in the United States each year. Such testing is widely regarded as being a key driver for clinical decisionmaking across healthcare organizations.1,2 Yet despite this acknowledged relationship, studies show that the use of lab testing is highly variable, and there is no correlation between lab test volume and patient outcomes.3
In fact, in addition to an estimated $200 billion wasted each year on excessive lab testing and treatment, overtesting and unnecessary transfusions can result in added risks to patients, and can lead to additional downstream testing and treatment that might not have been necessary.4
One study has shown that about 5% of healthy people receive test results that fall outside normal values, encouraging doctors to order additional tests and treatments that may not be needed.5 Such additional services cost US healthcare systems at least $210 billion a year, and contribute to 30,000 deaths annually.6,7

Figure 1. Since laboratorians are at the front line of ordering practices for both transfusions and clinical laboratory tests, they are well positioned to use utilization management systems to help change ordering behavior.
Similarly, blood transfusions are often overprescribed, are fraught with waste, and can increase patient risk. Between 1997 and 2011, red blood cell transfusions increased 134%, and a study has shown that about half of these transfusions were unnecessary, costing each hospital an average of $1 million annually.8 What’s more, blood transfusions carry risks, and have been associated with a 66% increased risk of mortality.9
It makes sense, then, for healthcare systems to implement test and transfusion utilization efforts that deliver the best patient outcomes, with the least risk, for the lowest cost. Since laboratorians are at the front line of ordering practices, they are poised to play a vital role in changing ordering behavior (Figure 1).
Blood Utilization Programs
Clinical laboratories can play an important role in reducing or eliminating unnecessary testing by spearheading or participating in hospital test and blood utilization efforts. Such initiatives combine the use of data insights and industry best practices to drive a culture of ordering only tests and procedures that improve patient outcomes, reduce waste, and contain costs.
The first step in implementing a test or blood utilization program is to gather a full understanding of the institution’s current system. It’s impossible to fix something without first understanding the problem, so any utilization program should begin by gathering, organizing, and analyzing the institution’s test ordering data. The result of this exercise can be eye-opening for health system executives, and is instrumental for building a case to garner internal support for change.
Dennis Spender, MD, medical director of McLaren Medical Laboratory, which supports the largest integrated health system in Michigan, recommends that utilization managers avoid the inclusion of too much detailed data in their reports, instead sharing analyses at a higher level of abstraction. Having implemented test and blood utilization programs at McLaren Health, Spender has learned that if the data and analyses provided are too granular, stakeholders may find them difficult to understand. “Worse yet, providers could feel they are being singled out by the data,” he says.
Instead, Spender suggests, utilization managers should zero in on which tests are being ordered, and the volume of tests ordered by the hospital system or department. This information becomes the beginning of fruitful conversations about why certain tests are being ordered, and whether there is a better process for determining which tests should be ordered. Keeping such data at a high level of abstraction enables health systems to turn the metrics into achievable objectives that can be measured.
Gathering such disparate data is a challenge for many health systems, as they lack the technologies needed to interoperate with disparate systems, gather their data, and prepare it for analysis. To solve this challenge, health systems are increasingly employing Cloud-based solutions capable of integrating with various data sources such as blood banks, clinical labs, and laboratory information systems (LISs). Such precision health platforms typically offer utilization management capabilities, gather and house data in a single repository, clean and organize the data, and deliver visual dashboards that make actionable metrics available to stakeholders for review.
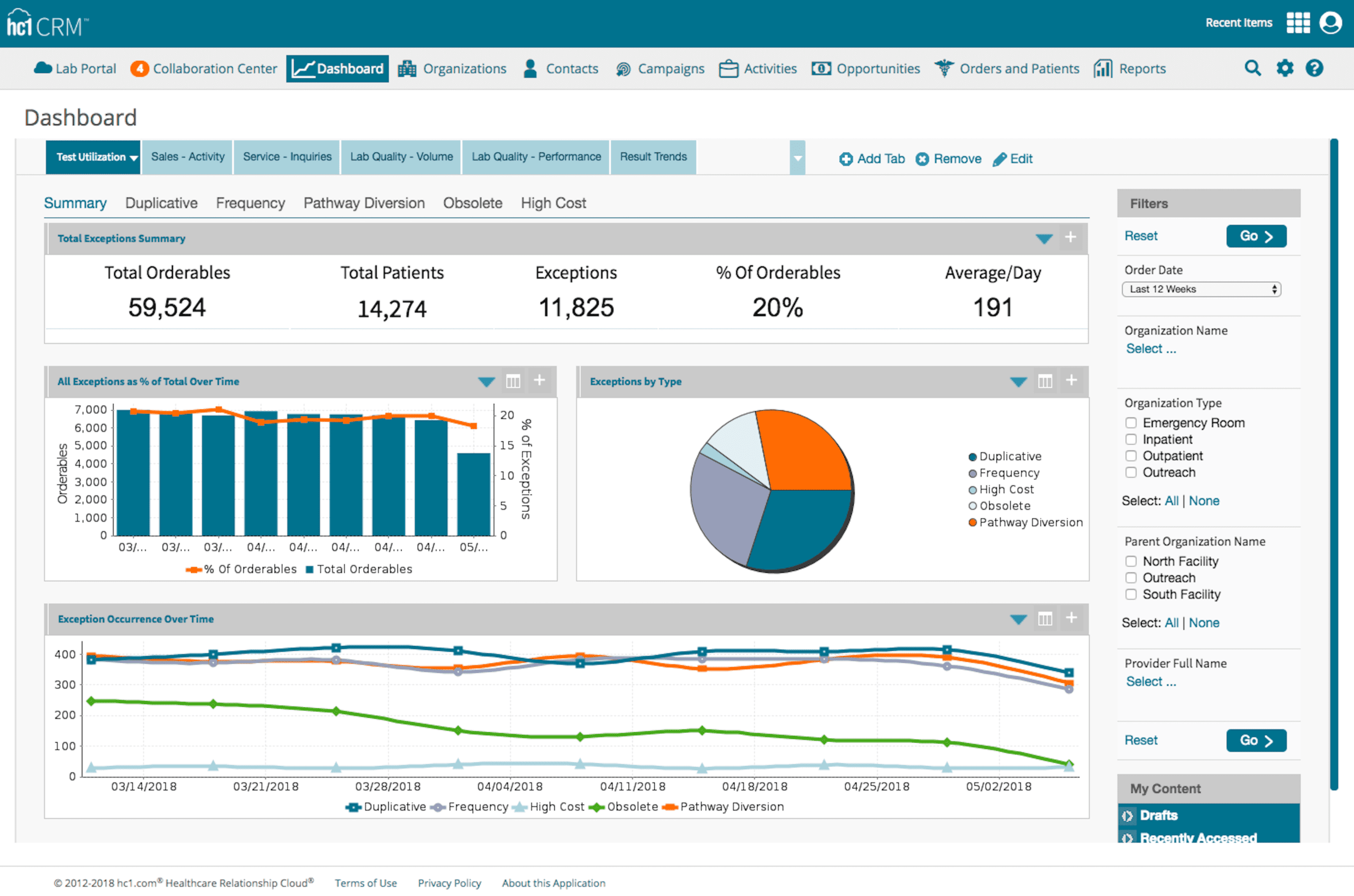
Figure 2. Sample test utilization dashboard showing lab testing metrics (click to enlarge).
Once health system leaders understand exactly how utilization processes are operating in their system, they should develop long-term goals for improved utilization programs based on professional society recommendations, such as those adopted by Choosing Wisely (http://choosingwisely.org), an initiative led by the American Board of Internal Medicine (ABIM) Foundation. Choosing Wisely is a multiyear effort to support and engage physicians to be better stewards of finite healthcare resources.
The Choosing Wisely list provides structure for five categories of utilization management:
- High-cost and unreimbursed testing.
- Unnecessary blood transfusions.
- Duplicative or repetitive tests.
- Clinical pathway diversions.
- Obsolete or unproven tests.

Figure 3. Sample dashboard showing blood utilization metrics (click to enlarge).
A test utilization management solution will have ready-to-go dashboards that conform to Choosing Wisely initiatives, and show test utilization data for metrics such as test send-outs for inpatient testing, test send-out volume month-over-month, payer mix for denials, absolute number of tests ordered, test ordering by physician, and screening by patient demographics, among others (Figure 2). For blood utilization programs, dashboards can showblood inventory and volume, C/T ratios, blood waste metrics, and appropriateness and exceptions. Such metrics enable clinicians to understand whether their institution’s transfusion processes are in line with industry standards (Figure 3).
Based on such information, health systems can begin utilization efforts by focusing on one or more areas for improvement, and then tackle additional improvements once success is achieved.
From Theory to Practice
McLaren Health identified blood utilization as its first reform initiative after discovering that the health system lagged in efficient blood usage compared to similar sized institutions. Over 3 years, McLaren Health’s blood utilization program resulted in an estimated cost savings of $37 million, including the cost to purchase and administer blood products, and to treat adverse reactions. Importantly, the health system estimates that the program saved 184 lives.
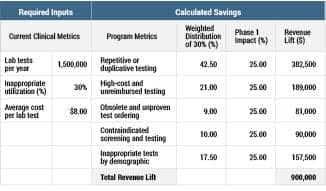
Table 1. Chart of test utilization reductions and cost savings from North Memorial Health Care, after the system adopted a test utilization program.
North Memorial Health Care (NMHC), a leading integrated healthcare system with more than 450 care providers serving 55,000 patients monthly, implemented a test utilization program as part of its shift from a volume-based payment model to a value-based system. The test utilization program set out to achieve four main priorities: population health, patient quality experience, operational efficiency, and profitable growth. The program enabled NMHC to reduce the number of unreimbursed tests by half, and resulted in estimated cost savings of $900,000 annually from reducing repetitive, duplicative, and inappropriate tests (Table 1).
To improve the chances of implementing a successful test utilization program, Spender recommends that health systems set up a utilization steering committee comprising system executives, medical lab directors, and providers. Members of such a group will contribute different perspectives on issues, and can make insightful observations to help the healthcare system prioritize its goals.
In order to drive changes in everyday clinical practice, blood and test utilization programs can adopt a variety of approaches, including hard stops—such as banning a test or not paying for unnecessary tests—as well as softer approaches, such as providing physician scorecards or intercepting orders for high-cost tests. A utilization management solutioncan help by triggering alerts that notify stakeholders when there is an incorrect use of a test (Figure 4).
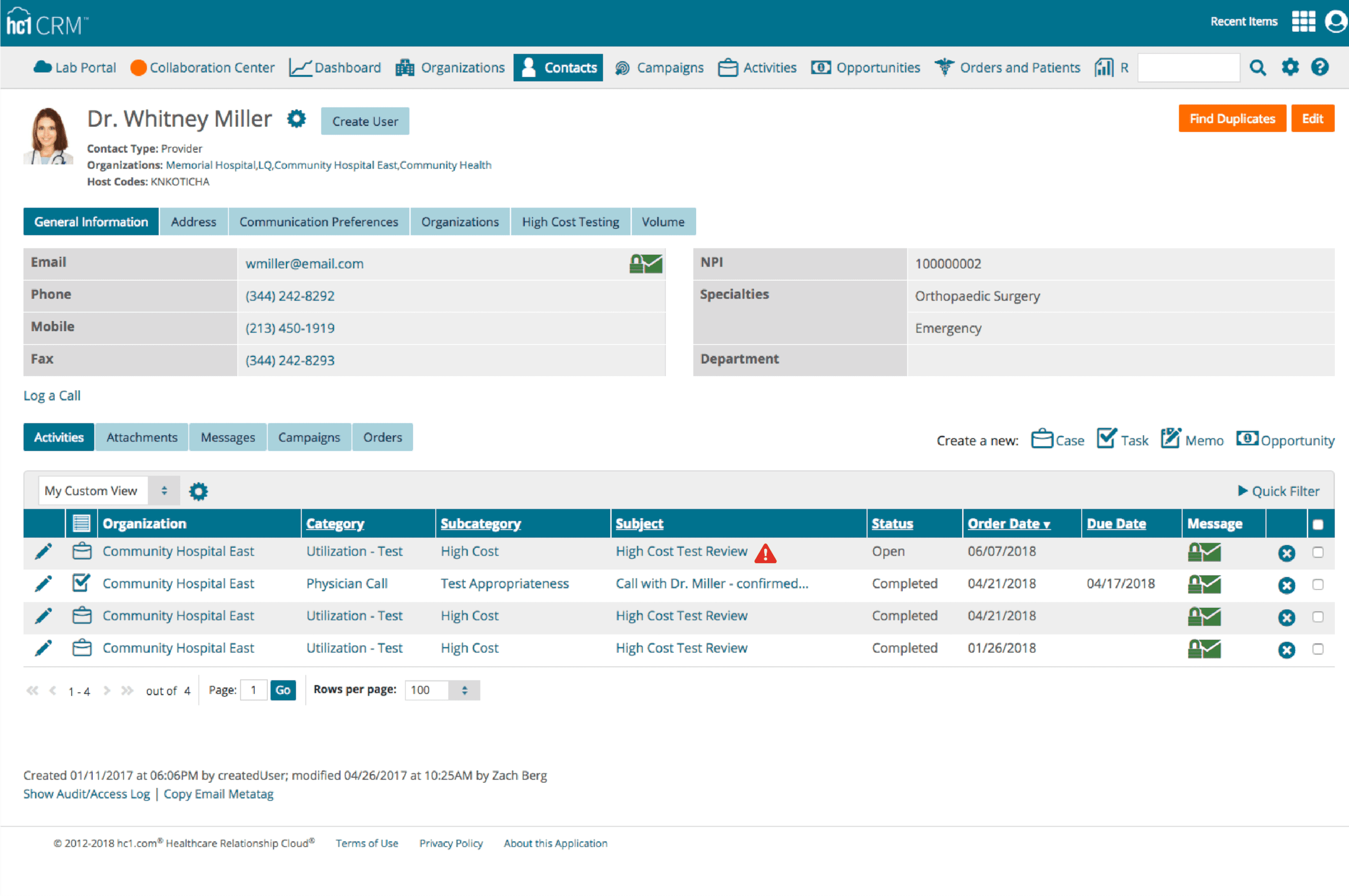
Figure 4. A blood or test utilization prompt can alert stakeholders to incorrect ordering of transfusions or lab tests (click to enlarge).
For example, Stanford Hospital and Clinics implemented a workflow in which a patient’s most recent lab results would be pulled up whenever a clinician requested blood through the hospital’s computerized ordering system. If the data indicated that the patient was healthy enough to get by without a transfusion, the doctor would receive a reminder of the guidelines and a request for justification for the order. After implementing the system, the number of red blood cell transfusions dropped by 24% between 2009 and 2013, representing an annual savings of $1.6 million in purchasing costs alone.10
Changing the Culture with Evidence
Changing clinical practice includes learning new best practices, while also deimplementing old practices. Education programs should therefore be an integral part of any utilization program. The ways that a test and blood utilization program is communicated and marketed to physicians can be an important factor in how readily the program is accepted. Merely implementing new procedures isn’t enough to win acceptance. Providers also need to understand why the program will help foster a culture of safe, patient-focused care.
When seeking the adoption of new clinical practice guidelines, for instance, the quality of the information that supports the guidelines greatly influences a physician’s decision about whether to accept the evidence, and change their behavior accordingly.11 Combining benchmark data about the current state of test ordering in a health system, together with information about public governance programs and best practices, delivers a strong, evidence-based approach that providers will understand and be more likely to support.
As utilization efforts unfold, utilization committees should regularly review progress. McLaren Health reports on progress monthly. This can easily be done by tapping into the real-time utilization dashboards to measure movement in key metrics. This progress should be disseminated to providers and health system executives, so that all stakeholders understand the value of these initiatives and can celebrate improvements.
Conclusion
Although laboratory testing itself accounts for only a tiny fraction of healthcare spending, it can trigger expensive downstream activities, such as imaging, prescriptions, surgeries, and hospital stays.12 Unlike lab tests, blood products are a limited commodity, which makes them pricey. It’s estimated that each unit of red blood cells costs $218, and this does not include overhead and transportation costs that can greatly increase the price.13
Since appropriate testing by definition supports a standard of care that leads to improved patient outcomes, one could argue that utilization efforts should lead to more cost-effective care. In today’s push for high-value healthcare, utilization efforts that will lead to better care at a lower cost to patients, payers, and health systems, are worthwhile endeavors.
Diane Janowiak is vice president for premium client solutions at hc1.com. Tim Hannon, MD, MBA, is CEO of Healthcare Forward. For further information, contact CLP chief editor Steve Halasey via [email protected].
References
1. Zhi M, Ding EL, Theisen-Toupal J, Whelan J, Arnaout R. The landscape of inappropriate laboratory testing: a 15-year meta-analysis. PLoS One. 2013;8(11):e78962; doi: 10.1371/journal.pone.0078962.
2. Alexander CB. Message from the president: reducing healthcare costs through appropriate test utilization. Critical Values. 2012;5(2):6–9; doi: 10.1093/criticalvalues/5.2.6.
3. Yeh DD. A clinician’s perspective on laboratory utilization management. Clin Chim Acta. 2014;427:145–150; doi: 10.1016/j.cca.2013.09.023.
4. Overuse 101 [online]. Brookline, Mass: Lown Institute, 2018. Available at: www.lowninstitute.org/learn/overuse-101. Accessed June 14, 2018.
5. Lab tests: get everything you need, but no more [online]. New Haven, Conn: Yale Medicine, 2018. Available at: www.yalemedicine.org/stories/avoid-unnecessary-lab-tests. Accessed June 14, 2018.
6. Szabo L. How unnecessary tests, scans, procedures and surgeries are affecting your patients [online]. Healthcare Finance. October 23, 2017. Available at: www.healthcarefinancenews.com/news/how-unnecessary-tests-scans-procedures-and-surgeries-are-affecting-your-patients. Accessed June 14, 2018.
7. Doctors speak out about unnecessary care as cost put at $800bn a year [online]. BMJ. October 2, 2012. Available at: www.bmj.com/press-releases/2012/10/02/doctors-speak-out-about-unnecessary-care-cost-put-800bn-year. Accessed June 19, 2018.
8. Jenkins I, Doucet JJ, Clay B, et al. Transfusing wisely: clinical decision support improves blood transfusion practices. Jt Comm J Qual Patient Saf. 2017;43(8):389–395; doi: 10.1016/j.jcjq.2017.04.003.
9. Czajka R. Are you using too much blood? Curbing unnecessary blood transfusions [Action for Better Healthcare blog, online]. Charlotte, NC: Premier Inc, 2018. Available at: www.actionforbetterhealthcare.com/using-much-blood-curbing-unnecessary-blood-transfusions.Accessed August 6, 2018.
10. Anthes E. Evidence-based medicine: save blood, save lives. Nature. 2015;520(7545):24–26; doi: 10.1038/520024a.
11. Gupta DM, Boland RJ Jr, Aron DC. The physician’s experience of changing clinical practice: a struggle to unlearn. Implement Sci. 2017;12(1):28; doi: 10.1186/s13012-017-0555-2.
12. Song Z, Safran DG, Landon BE, et al. Healthcare spending and quality in year 1 of the alternative quality contract. N Engl J Med. 2011;365(10):909–918; doi: 10.1056/NEJMsa1101416.
13. Kacik A. Hospitals see improved outcomes, lower costs as blood transfusions drop. Modern Healthcare. July 21, 2017. Available at: www.modernhealthcare.com/article/20170721/news/170729977. Accessed August 6, 2108.




{kind=link}