
The accuracy of prostate-specific antigen (PSA) in prostate cancer screening can be improved by accounting for genetic factors that cause changes in PSA levels that are not associated with cancer, according to a multi-center study led by UC San Francisco and Stanford University.
In a study publishing June 1, 2023 in Nature Medicine, UCSF researchers and their collaborators conducted a large genome-wide association study of PSA in more than 95,000 men without diagnosed prostate cancer, which identified over 80 novel PSA-associated variants. They set out to discover whether accounting for genetic factors that cause variations in the levels of PSA that are not attributable to cancer could help improve prostate cancer screening.
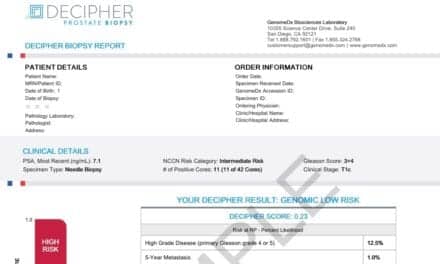
“PSA levels represent the main diagnostic biomarker for prostate cancer. This test is widely used but not currently implemented as part of a formal screening program,” says Linda Kachuri, PhD, MPH, a former postdoctoral scholar in the Department of Epidemiology & Biostatistics at UCSF and lead author of the study. “Because of its poor sensitivity and specificity, PSA testing can often lead to detecting latent disease or, in some cases, missing aggressive tumors.”
The researchers leveraged these new data to build a genome-wide polygenic score for PSA, measuring an individual’s genetic predisposition based on genetic variations.
“The polygenic score captured each individual’s genetic predisposition to high PSA levels,” says Rebecca Graff, ScD, UCSF assistant professor in the Department of Epidemiology & Biostatistics and one of the senior authors of the study. “The polygenic score was strongly associated with PSA levels in validation cohorts and was not associated with prostate cancer, confirming that it reflects benign PSA variation.”
To examine whether the polygenic score could improve the detection of clinically significant disease and reduce overdiagnosis, the researchers applied the polygenic score correction factor to a real-world Kaiser Permanente cohort and estimated the effects of this adjustment on the PSA thresholds used for biopsy referrals.
“We adjusted each person’s PSA values based on his unique genetic profile,” explained Kachuri. “PSA values personalized in this way are more likely to reveal changes in PSA due to prostate cancer because they are corrected for the influence of inherited genetics.”
Applying a correction to PSA levels improved the accuracy of biopsy referral decisions. Roughly 30% of men could have avoided biopsy, though adjusted PSA levels would have missed approximately 9% of positive biopsies. Most of the latter cancers were low-grade disease that did not require treatment, but there remains room to improve the polygenic score.
“We showed that genetic correction of PSA levels has the potential to both reduce unnecessary biopsies and improve our ability to detect tumors with a more aggressive profile,” says Kachuri. “We hope that our findings represent a step forward in developing informative screening guidelines and reducing the diagnostic gray area in PSA screening.”
While the study was very large, almost 90% of the participants were of predominantly European ancestry. According to Kachuri, this represents a key limitation because the composition of the study doesn’t fully reflect the patient population impacted by prostate cancer. “We hope to be able to share findings soon from our efforts to conduct larger and more diverse studies of PSA genetics,” she said.

{kind=link}