
Current and emerging cardiac markers signal improved testing for better patient outcomes
By Craig C. Foreback, PhD
Cardiovascular diseases continue to be the leading cause of death in the United States, responsible for nearly 800,000 deaths annually—or about one in every three deaths. Heart disease is the leading cause of death for both men and women, claiming the lives of about 610,000 Americans each year.1 Coronary artery disease is the most common type of heart disease, killing more than 370,000 people annually.
In addition, about 5.1 million people in the United States have heart failure.2 About half of the people who develop heart failure die within 5 years of diagnosis. In 2009, one out of every nine deaths included heart failure as a contributing cause. Heart failure costs the nation an estimated $32 billion each year.
In light of such dire statistics, it’s no wonder that achieving speedy diagnosis of acute myocardial infarction (AMI)—heart attack—remains a significant concern in emergency departments throughout the nation. Early triage of patients to rule-in or rule-out AMI is challenging. For many years, testing for the presence of the regulatory proteins troponin I or troponin T—both released into the bloodstream when the heart muscle has been damaged—has been the gold standard for diagnosing AMI. But recent reports have indicated that the latest generation of high-sensitivity troponin tests can increase diagnostic efficiency and improve early diagnosis of myocardial infarction.
AMI AND HIGH-SENSITIVITY TROPONIN TESTS

Alere’s troponin I test is a cartridge-based high-sensitivity immunoassay.
The current interest in high-sensitivity (hs) methods for detecting troponin extends to both troponin I and troponin T, and there are hs-troponin assays for detecting both proteins. “There are some differences between troponin I and troponin T,” says Thomas Koshy, PhD, director of scientific affairs at Alere, Waltham, Mass, “but so long as one is aware of the differences, both markers are suitable for detecting myocardial necrosis.”
Although hs-troponin tests have been shown to have impressive capabilities, “they are not entirely new tests, as sometimes described in the lay press,” says Koshy. “The high-sensitivity assays detect the same biomarkers as conventional troponin assays, but with greatly improved sensitivity and precision at low concentrations.”
Older tests were not able to detect low levels of troponin, Koshy explains, so any positive result indicated significant cardiac damage. By contrast, high-sensitivity methods can detect very low levels of troponin, and the better ones are even able to detect circulating troponin in normal patients. “This capability made it necessary to establish a reference range for high-sensitivity assays at the 99th percentile of normal,” says Koshy. “In turn, this resulted in the redefinition of AMI as indicated by any troponin level above the 99th percentile, when accompanied by signs and symptoms of cardiac ischemia.”

Margot LeClair, Beckman Coulter Diagnostics.
“The new generation of hs-troponin assays offers a number of exciting advances,” says Margot LeClair, global products manager at Beckman Coulter Diagnostics, Brea, Calif. “But the key performance feature that broadens the utility of the tests is their increased sensitivity, which leads to better precision.”
High-sensitivity troponin tests offer several advantages over older troponin tests. To begin with, they make it possible to identify a greater number of patients who are not experiencing an AMI, providing physicians with greater confidence in ruling-out AMI for a patient presenting to the emergency department with chest pain. When such a patient presents without signs or symptoms of cardiac ischemia, an hs-troponin result below the 99th percentile is evidence that the patient is not experiencing an AMI.
This evidence is even stronger if the patient has sequential negative results over a 2- to 6-hour period. But it has been a challenge to determine the significance of changes observed in serial testing when using older troponin tests.
“High-sensitivity troponin assays should clear up some of the uncertainties that physicians are faced with today,” says LeClair. “With an improved ability to detect significant change between serial measurements, it becomes possible to achieve higher diagnostic accuracy for the diagnosis of AMI.
“High-sensitivity assays measure the 99th percentile upper reference limit of the healthy population with a coefficient of variation less than 10%,” observes LeClair. “The high precision of these assays increases their ability to determine small differences in troponin level over time, leading to a better definition of significant change between serial measurements.
“With high-sensitivity assays, protocols that enable physicians to rule-out an AMI within 1 to 2 hours of the patient presenting to the emergency department are now possible,” adds LeClair. “Providing a safe path to early discharge for patients who do not have acute coronary syndrome helps to alleviate duplication of work and emergency department overcrowding that can lead to undesirable patient outcomes.”

Performed on the company’s Stratus CS 200 acute care cardiac analyzer, available in Europe, the cTnI test by Siemens Healthcare meets guideline recommendations of ?10% CV at the 99th percentile of a normal population.
A recent study concluded that an elevated cardiac troponin level detected by a high-sensitivity test for either troponin I (hs-cTnI) or troponin T (hs-cTNT) was highly predictive of all-cause death. The study found that the hs-cTnI test was more specific, but the hs-cTnT test was more predictive of adverse events.3
A disadvantage of both hs-troponin tests is that they make it more difficult to rule-in AMI. A positive hs-troponin test is no longer an automatic rule-in for AMI, so identifying the cause of an elevated hs-troponin test can lead to increased utilization of other diagnostic procedures. “One way to sort out these patients is to make use of a serial testing algorithm,” says Koshy. “By this method, the physician would order an hs-troponin test at presentation to the emergency department, and then again at 1, 2, and 3 hours after presentation.” Two recent reports concur with this recommendation.4,5
TROPONIN BEYOND AMI
High-sensitivity troponin assays can also detect abnormal levels of troponin caused by heart failure, cardiac myopathies, and end-stage renal disease. “With more research, hs-troponin assays may be found to have utility for more than the diagnosis of AMI,” says Koshy.

The troponin I test by Alere runs on the company’s Triage MeterPro.
Recent research has suggested that high-sensitivity troponin assays may be useful in guiding the treatment of heart failure. In one study among patients at risk for cardiomyopathy secondary to high-dose chemotherapy, elevated troponin levels were found to be associated with deterioration of cardiac function.6 In another study, higher troponin T levels were associated with increased cardiovascular risk, and especially with heart failure.7 Consequently, it is believed that hs-troponin tests could be useful in determining which patients might benefit from earlier intervention, and in guiding further disease management.
An increasing number of publications are investigating the use of high-sensitivity troponin tests among heart failure patients not for diagnosis, but for prognosis. Circulating troponins, for instance, are believed to offer significant prognostic value for patients with heart failure. A recent study reported that an hs-cTnT test provided accurate prognostic information and increased prognostic utility when compared with an hs-cTnI test. In fact, the hs-cTnT test correctly predicted a two-fold increase in mortality and associated increased hospitalizations for heart failure.8
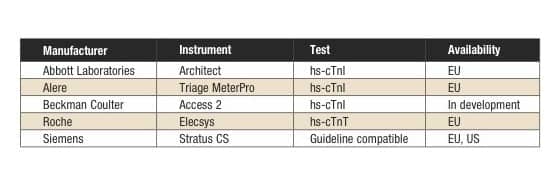
Table 1. Status of commercial high-sensitivity troponin tests in the United States and Europe. Click to expand.
Tests conforming to the guidelines for high-sensitivity troponin I testing are available in the United States from Siemens Healthcare, Tarrytown, NY, and in Europe from Abbott Laboratories, Abbott Park, Ill; Alere; and Siemens. Beckman Coulter is developing its own version of such a test. Roche Diagnostics, Indianapolis, is the only manufacturer of an hs-troponin T test, which is available in Europe, but not in the United States (see Table 1).
NATRIURETIC PEPTIDES
Natriuretic peptides are the accepted markers for diagnosing heart failure and predicting cardiovascular events in patients with coronary artery disease. B-type natriuretic peptide (BNP) is a cardiac hormone secreted by cardiac myocytes in response to ventricular wall stress secondary to volume and pressure overload. Its diuretic, natriuretic, and vascular effects alleviate many of the detrimental consequences of heart failure.
BNP begins as a 134 amino acid, preproBNP, which splits into a 108 amino acid, proBNP, and a signal peptide. When secreted, the propeptide is proteolytically cleaved to form the 32 amino acid active hormone BNP, which promotes sodium and water excretion, and an inactive 76 amino acid, N-terminal pro B-type natriuretic peptide (NT-proBNP).

Thomas I. Koshy, PhD, Alere Inc.
“The flagship markers for heart failure are BNP and NT-proBNP, and this will not change in the near future,” says Koshy. Although the two peptides are secreted in a 1:1 ratio, they differ from one another in several significant ways. BNP is cleared from the body by binding to receptors and neutral endopeptidase, and has a half-life of just 20 minutes. By contrast, NT-proBNP is cleared from the body by the kidneys, and has a longer half-life of 90 to 120 minutes. These differences explain the different serum concentrations of BNP and NT-proBNP in patients with acute decompensated heart failure.
Despite their differences, both BNP and NT-proBNP serve as clinically validated biomarkers for the diagnosis, treatment, and prognosis of heart failure, and both are incorporated into national and international medical guidelines for heart failure.9 It was initially thought that the active BNP molecule should be the preferred marker. However, numerous publications validate the use of both natriuretic peptides in the diagnosis and prognosis of heart failure and in biomarker-guided therapy, dispelling concern that NT-proBNP measurements might be affected when testing patients with chronic renal failure.10–13
But not every drug behaves the same way. “The newest drug for the treatment of heart failure is Entresto (sacubitril/valsartan) from Novartis,” says Frederick Kiechle, MD, PhD, chairman and director of clinical pathology at Memorial Regional Hospital, Hollywood, Fla. “The use of natriuretic peptides with Entresto is a quite a hot topic, because one of the compounds in the drug inhibits the degradation of BNP.”
Thus, taking Entresto could result in an increased BNP level, even though the patient is getting better. But on the other hand, Entresto has no effect on the metabolism of NT-proBNP, so the concentration of that marker would fall as the patient’s heart failure improves.
Such differences in uptake suggest that both BNP and NT-proBNP should be monitored when Entresto is used for the treatment of heart failure. However, more studies need to be done to fully understand how the natriuretic peptides react to Entresto.
NEW MARKERS ON THE WAY
Researchers are continuing to develop new markers for the diagnosis and prognosis of heart failure. A recent addition to the group is galectin-3, which is a b-galactoside lectin member of the galectin family. Levels of circulating galectin-3 are increased in heart failure patients, and testing of the levels has been shown to be useful for risk stratification of patients. Testing for galectin-3 was included in the 2013 guidelines for the management of heart failure compiled by the American College of Cardiology Foundation and the American Heart Association.14
An automated assay for circulating levels of galectin-3 is available in the United States. BG Medicine, Waltham, Mass, has developed a quantitative enzyme-linked immunosorbent assay on a microtiter plate platform that measures galectin-3 in serum or plasma. BG Medicine has also partnered with Abbott Laboratories to develop its galectin-3 test for use on Abbott’s Architect automated platform.15

The first automated test for galectin-3 joined the cardiac test menu of the Architect Plus i2000sr immunoassay analyzer by Abbott Laboratories in July 2015.
A recent study evaluated the clinical validity and cost-effectiveness of the Architect galectin-3 assay.16 The study demonstrated that galectin-3 levels were related to the severity of heart failure, based on the New York Heart Association functional classes. Galectin-3 levels higher than 19.2 ng/ml were predictive of long-term cardiovascular death of patients with systolic heart failure. The study also estimated that the Architect assay improved diagnostic related group reimbursement by as much as 15%.
CONCLUSION
Together with the availability of new drugs, recent developments in diagnostic testing for cardiac ischemia and heart failure have helped to improve outcomes for patients with cardiovascular diseases. High-sensitivity troponin tests have improved the certainty of ruling-out AMI, and have led to the identification of more patients who have experienced myocardial infarction. And while researchers are continuing to identify and develop additional markers indicative of cardiovascular health and disease, new markers such as galectin-3 are improving outcomes in patients with heart failure.
Craig C. Foreback, PhD, is a contributing writer and member of the CLP editorial advisory board. For further information, contact chief editor Steve Halasey via [email protected].
REFERENCES
- CDC Wonder: about underlying cause of death, 1999–2014 [online]. Atlanta: Centers for Disease Control and Prevention, National Center for Health Statistics, 2015. Available at: http://wonder.cdc.gov/ucd-icd10.html. Accessed February 10, 2016.
- Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics, 2013 update: a report from the American Heart Association. Circulation. 2013;127(1):e6–e245; doi:10.1161/cir.0b013e31828124ad.
- Cullen L, Aldous S, Than M, et al. Comparison of high-sensitivity troponin T and I assays in the diagnosis of non-ST elevation acute myocardial infarction in emergency patients with chest pain. Clin Biochem. 2014;47(6):321–326; doi: 10.1016/j.clinbiochem.2013.11.019.
- Cullen L, Mueller C, Parsonage WA, et al. Validation of high-sensitivity troponin I in a 2-hour diagnostic strategy to assess 30-day outcomes in emergency department patients with possible acute coronary syndrome. J Am Coll Cardiol. 2013;62(14):1242–1249; doi: 10.1016/j.jacc.2013.02.078.
- Body R, Carley S, McDowell G, Jaffe AS, et al. Rapid exclusion of acute myocardial infarction in patients with undetectable troponin using a high-sensitivity assay. J Am Coll Cardiol. 2011;58(13):1332–1339; doi: 10.1016/j.jacc.2011.06.026. Erratum in: J Am Coll Cardiol. 2012;60(12):1122.
- Cardinale D, Sandri MT, Colombo A, et al. Prognostic value of troponin I in cardiac risk stratification of cancer patients undergoing high-dose chemotherapy. Circulation. 2004;109(22):2749–2754.
- Pokharel Y, Sun W, de Lemos JA, et al. High-sensitivity troponin T and cardiovascular events in systolic blood pressure categories: atherosclerosis risk in communities study. Hypertension. 2015;65(1):78–84; doi: 10.1161/hypertensionaha.114.04206.
- Grodin JL, Neale S, Wu Y, et al. Prognostic comparison of different sensitivity cardiac troponin assays in stable heart failure. Am J Med. 2015;128(3):276–282; doi: 10.1016/j.amjmed.2014.09.029.
- Santaguida PL, Don-Wauchope AC, Oremus M, et al. BNP and NT-proBNP as prognostic markers in persons with acute decompensated heart failure: a systematic review. Heart Fail Rev. 2014;19(4):453–470; doi: 10.1007/s10741-014-9442-y.
- Troughton R, Felker GM, Januzzi JL Jr. Natriuretic peptide-guided heart failure management. Eur Heart J. 2013;35:16–24; doi: 10.1093/eurheartj/eht463.Advance access published November 11, 2013.
- Gaggin HK, Mohammed AA, Bhardwaj A, et al. Heart failure outcomes and benefits of NT-proBNP-guided management in the elderly: results from the prospective, randomized proBNP outpatient tailored chronic heart failure therapy (PROTECT) study. J Card Fail. 2012;18(8):626–634; doi: 10.1018/j.cardfail.2012.05.005.
- Felker GM, Ahmad T, Anstrom KJ, et al. Rationale and design of the GUIDE-IT study: guiding evidence-based therapy using biomarker intensified treatment in heart failure. JACC Heart Fail. 2014;2(5):457–465; doi: 10.1016/j.jchf.2014.05.007.
- Gaggin HK, Szymonifka J, Bhardwaj A, et al. Head-to-head comparison of serial soluble ST2, growth differentiation factor-15, and highly-sensitive troponin T measurements in patients with chronic heart failure. JACC Heart Fail. 2014;2(1):65–72; doi: 10.1016/j.jchf.2013.10.005.
- Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. J Am Coll Cardiol. 2013;62(16):e147–e239; doi: 10.1016/j.jacc.2013.05.019.
- Automated galectin-3 test [online]. Waltham, Mass: BG Medicine, 2015. Available at: www.bg-medicine.com/automated-galectin-3-test. Accessed February 4, 2015.
- Gruson D, Mancini M, Ahn SA, Rousseau MF. Galectin-3 testing: validity of a novel automated assay in heart failure patients with reduced ejection fraction. Clinica Chimica Acta. 2014;429:189–193; doi: 10.1016/j.cca.2013.12.017.




{kind=link}