
Breathalyzer technology offers a number of diagnostic advantages, including being non-invasive, requiring minimal training of testing personnel, and delivering results in just minutes. CLP recently sat down with Liesbet Lagae, program director of life sciences for imec, to discuss how breathalyzer technology could be a diagnostic game changer.
By Chris Wolski
With clinical diagnostics rapidly responding to the ongoing COVID-19 pandemic, it’s not surprising that there have been and will likely continue to be breakthroughs in testing technology. One technology, which is being developed by imec relies on breathalyzer technology to identify infected and infectious people.
CLP recently sat down with Liesbet Lagae, PhD, imec fellow and program director of life science technologies for the company, to discuss the company’s breathalyzer technology, its advantages, and how it could be applied to other disease states.
Lagae’s career has been marked by leading diagnostic innovations, including initiating the field of molecular and cellular biochips at imec that have resulted in smart chip solutions to the life science industry. Applications for these chips include point-of-care diagnostics, DNA sequencing and storage, cytometry, bioreactors, and implants. Lagae has authored or co-authored more than 250 peer-reviewed journal articles, and 20 patents. She also holds a part-time appointment in nanobiotechnology at KU Leuven’s physics department, where she received her PhD.
Lagae’s answers have been edited for length and clarity.
CLP: Your COVID test is significantly different than what has been established as the gold standard—can you explain how you based your approach on breathalyzer technology and what advantages this provides?
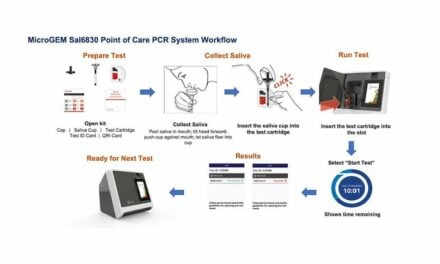
Liesbet Lagae: We capture aerosols from exhaled breath and we are able to detect virus in these aerosols via both standard and ultra-fast PCR. The same aerosols are the main source of transmission between persons. The advantages include non-invasive sampling—which is easy to do on a daily basis—fast time to result, about 15 minutes in our demonstrator, and the identification of infectious persons as opposed to infected persons.
CLP: One of the advantages, as I understand it, is the collection side of the testing. Your breathalyzer technology does not require trained medical professionals to collect the samples. How does this improve testing?
Lagae: The sampling success depends on the used breathing method. We can steer the breathing behavior via a feedback system and highlight failed tests. The training of the medical professionals or other testing personnel has very little impact on the result, as opposed to a nasopharyngeal swab, where the results vary strongly between different assistants.
CLP: While you’re able to provide rapid results—how scalable are they? In other words, how many tests can you process in 15 minutes?
Lagae: This requires some nuance: the current demonstrator handles 1 sample in 15 minutes. Two samples in parallel requires two full blown instruments side by side. A next iteration should be more adapted to commercial use: speed can be increased to below 10 minutes and the core of the instrument can be made modular. To go to one sample per minute to match the sampling speed you would need 10 modules in parallel.
CLP: How are clinical labs involved in providing results?
Lagae: Today, imec generates the breath sampling results, trained medical personnel from the university hospital take the tests, and the standard clinical laboratory runs the reference nasopharyngeal swab samples. For a commercial product, it depends on the regulation and product labeling if a clinical lab is required to generate or release the results.
CLP: Your breathalyzer technology is joining a plethora of other COVID tests. How does having a menu of tests to choose from help providers, labs, and patients?
Lagae: The market will settle on fewer tests in the future. Some test types are not as good as they’re assumed to be and others will be too expensive in the long term. We believe breath sampling will gain its place as a commonly used test.
CLP: It’s my understanding that you see your COVID breathalyzer technology as just the first of a set of breathalyzer tests that you have on the drawing board. Can you discuss the potential for breathalyzer tests and how they’ll impact or change clinical laboratory workflows?
Lagae: First on the list are other respiratory infectious diseases, such as tuberculosis, RSV, and influenza. But we know the aerosols also contain highly concentrated and “clean” human material such as RNA, DNA, and proteins. We believe this can be used for diagnosis of a range of pathologies, in the same way blood or serum is used today.
CLP: Is your breathalyzer test available commercially? If not, when do you expect it to be available?
Lagae: A first version of the technology, which is not integrated with PCR, should be available in 2022 via a startup. The integrated PCR and other applications will follow.
Chris Wolski is chief editor of CLP.


{kind=link}