
Serology testing for SARS-CoV-2 will be beneficial and potentially even necessary in assessment of vaccine effectiveness
By Kalen N. Olson, PhD, and Katherine Soreng, PhD
In clinical practice, quantitative antibody testing for assessing the need to vaccinate/boost is common, especially in cases such as hepatitis B vaccination, where the neutralizing surface antigen-antibody threshold associated with immunity is known.1 In population-based studies, SARS-CoV-2 antibody testing has been shown to identify a significant percentage of the population with an immune response to the virus but undiagnosed for covid-19.2-6 Commercially available clinical laboratory serology testing suitable for clinical practice is not expensive and can often be high-throughput, with fast turnaround and broad population access. While many serology assays that came to market initially were of low quality given the initial interest in facilitating an immediate, even if suboptimal, testing capability during the outset of the pandemic, increased regulatory expectations have effectively removed low quality assays from authorized lists. Currently available assays with very high (≥99.5%) specificity, particularly important under conditions of low disease prevalence, will be essential to vaccination campaigns, both to identify vulnerable populations as well as assess for a successful response in large populations.7,8
As learned during this pandemic for other types of SARS-CoV-2 testing, such as PCR, availability at a large and accessible scale is key to ensuring that the needs of the population can be met. While proof of antibody- associated immunity in SARS-CoV-2 is emerging from the vaccine trials and other datasets, extensive data to date already support a role for neutralizing antibody in protecting from (or mitigating) infection.9-17
Studies from natural infections indicate significant diversity in the levels and duration of neutralizing antibody responses, with declining levels over time potentially leading to reinfection.17-26 Consequently, testing is essential to distinguish successful from suboptimal vaccine responses and detect antibody declines after natural infection.27-29 The factors influencing likelihood of a robust neutralizing antibody response are poorly defined but have been linked to immunocompetency, age, and disease severity.27,30,31 Existing data indicates that detectable levels of circulating neutralizing antibody are necessary for protection, though the role of memory B-cells and/or T-cells is still under investigation.
Considerations
Antibody-mediated immunity
Immune responses to pathogens are diverse and involve both adaptive and innate elements.32,33 Adaptive immunity is pathogen-specific and principally mediated by B- and T-cells. Humoral immunity is driven by B-cells that produce antibody (often “helped” by T-cells that secrete specific cytokines). With many pathogens, antibodies are the principal effector of protection, particularly if they can block (neutralize) viral entry.34Because antibody-mediated viral neutralization is often, but not always, a correlate for immunity, confirmed protection in vivo associated with specific antibodies/ levels must be established. A growing body of data supports the potential for neutralizing antibody to confer protection from SARS-CoV-2.9-17,35-37 This includes both in vitro demonstrations of antibody neutralization and in vivo evidence in a range of experimental animal models challenged with live virus. While conflicting data exists on the duration of neutralizing antibodies following SARS-CoV-2 infection, increasing datasets suggest persistence in excess of 3 months in the majority of infections, including those with mild or moderate disease.17,20,21,24,38-41 As vaccine-induced production of neutralizing antibodies proves effective, assessment of neutralizing antibody levels to identify/confirm a protective threshold will be vital in establishing broad population-based immunity.
Vaccine-related serology test applications
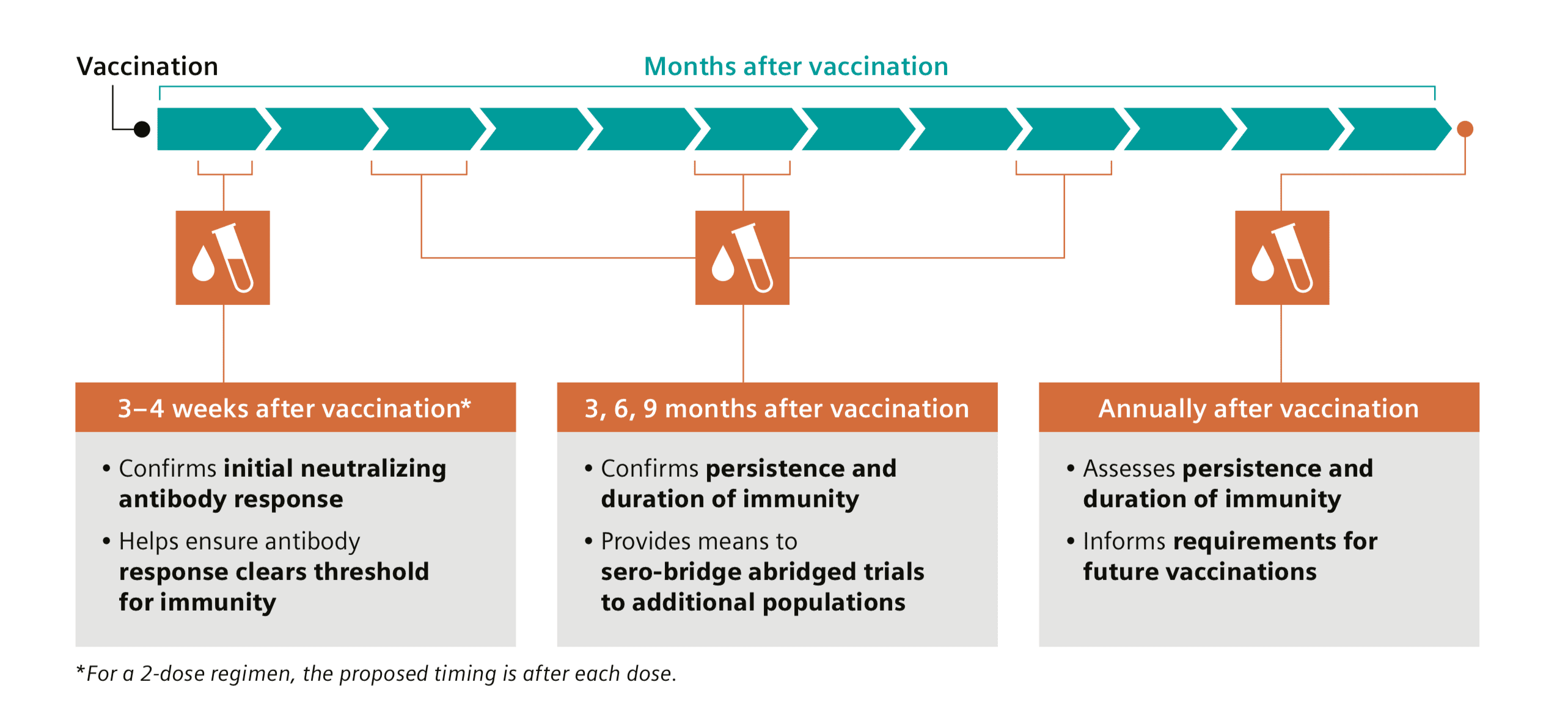
Vaccination-related testing for neutralizing antibody can be used at multiple timepoints. Ongoing clinical trials for recently authorized vaccines, and vaccines in development, are utilizing serology testing for neutralizing antibody titer as a surrogate of efficacy.15,16,27,37,42-57 These trials are assessing neutralizing antibody immunogenicity in response to vaccine administration over time, which will be necessary to inform antibody-mediated protection. A modeling study assessing vaccine prioritization strategies demonstrated there may be value in pairing serology testing with vaccination in areas with higher SARS-CoV-2 seroprevalence.58 As current vaccines require a two-dose regimen to broadly stimulate levels of neutralizing antibody, serology testing would measure for an effective response approximately 3 to 4 weeks after each dose.37,59 For logistical convenience, in many settings serology testing can be undertaken during the same visit as the second vaccine dose administration. Quantitative periodic antibody testing post-vaccination, after approximately 3, 6, and 9 months, would ensure a sustained antibody response at sufficient levels for virus neutralization (Figure 1). Initially, additional data on duration of antibody-mediated protection is needed across populations, and in the long-term testing may be focused on particular populations with known risk of insufficient immune response. The timing of appropriate serology testing would be optimized and refined as needed. A serology-defined threshold (from either natural infection or vaccination) remains a key need, and this periodic testing would offer additional data on antibody response patterns to determine optimal serology testing utilization. Longer-timeframe quantitative testing for waning levels of protective antibody, such as through annual testing, would inform the need to revaccinate/boost.
Antibody targets and neutralization
Current commercially available SARS-CoV-2 antibody assays have diverse targets, including nucleocapsid (N) protein, whole spike (both S1 and S2 regions), S1, and S1-RBD.39-63 Robust evidence in vitro and from animal model studies supports a mechanism of viral neutralization by antibodies to the spike glycoprotein, primarily through inhibition of recognition/attachment to the ACE2 host cell receptor. While several epitope-specific neutralizing spike antibodies have been identified (in both S1 and S2), most target the S1-RBD, as these antibodies can interfere with recognition and binding to ACE2.9-11,17,38 Since both whole-spike- and S1-targeted assays include the RBD region, they can indicate, but not specifically identify, the presence of RBD-associated neutralizing antibodies. S1-RBD-specific assays are likely to prove advantageous over S1 and whole spike, especially if using a quantitative assay, as neutralizing versus binding antibodies might be expected to be enriched and therefore a better correlate to immunity. While not all antibodies to the RBD are equally neutralizing, the RBD is identified as the immunodominant source. Depletion analysis indicates an estimated ~90% of known neutralizing antibodies target epitopes within the RBD.10,17,35 While current data on S1-RBD vaccines may preclude the need for changes to vaccine design, second-generation vaccines may use a broader set of antigenic targets.
Quantitative versus qualitative reporting
Current SARS-CoV-2 qualitative antibody assays have a defined cut-point based on presence/absence of immune response rather than a threshold value based on antibody level and neutralization of the virus. Therefore, they only provide a “yes” or “no” indication of a response to infection. Quantitation of neutralizing antibody supports identification of an immune threshold, above which individuals are likely to be protected and below which they are susceptible. A few IgG and total antibody quantitative assays for the spike protein (including the S1-RBD) are already commercially available.64-67 Antibodies to SARS-CoV-2 can decline quickly and at different rates for different epitopes,18,19,20,22,24 so quantitation would prove salient for rapid assessment of immunity or need to boost. Quantitative testing would be a valuable tool for establishing a protective threshold, as well as initial assessment of vaccination response and monitoring of antibody levels over time when a threshold is established.
Vaccines and efficacy in current clinical trials
In phase 3 vaccine trials, protection from disease, i.e., immunity, has been demonstrated relative to the placebo group despite a finite incidence of infection in the vaccinated subjects. A vaccine could achieve statistical significance for the primary endpoint for protection from disease despite significant incidence of disease in the vaccinated group.68 Even with high efficacy, a proportion of those inoculated would not have protection from disease. Assessment for seroconversion failure or declining levels in the vaccinated but susceptible population is a critical parameter with implications for patient care, population management, and public policy.5,69 Data from initial vaccine trials is limited to certain populations and exposure patterns. Additional data on antibody response and duration will be needed to help inform vaccine efficacy in larger, more-diverse populations to determine appropriate use in the context of variables such as vaccine design/manufacturer, ethnicity, level of viral load exposure, and individual immune system strength. All vaccines in use or development published on to date include or are based solely on the spike protein, with spike- or RBD-specific antibodies serving as a surrogate of efficacy along with elements of the cellular response. In this scenario, natural infection can be monitored by testing for antibody to the N protein. However, testing for quantitative S1-RBD antibodies would be the preferred method to assess levels relative to susceptibility following vaccination due to their correlation to neutralization and protection. Additional data on vaccine use and antibody response in already- seropositive patients is needed to determine response patterns in a more-diverse antibody population.
Summary
To enable an effective vaccination strategy, Siemens Healthineers advocates for the use of automated SARS- CoV-2 serology testing to help confirm efficacy.
Serology assays should have the appropriate characteristics for assessment of vaccine response:
- Quantitative results
- S1-RBD-neutralizing IgG antibody detection
- Very high (≥99.5%) specificity
Serology testing can inform vaccination utilization and status of protection at multiple junctures:
- Post-vaccination initial response after approximately 3 to 4 weeks (after each dose)
- Duration of vaccination response after approximately 3, 6, and 9 months and annually (need to boost)

Additionally, quantitative neutralizing-antibody testing could support determination of an antibody threshold for immunity/susceptibility to SARS-CoV-2 and provide critical data needed to understand vaccine-facilitated antibody response and duration in populations not included in initial vaccine trials. Serology is a cost-effective surrogate for vaccine efficacy and able to meet high-volume testing needs. Ensuring the effectiveness of vaccines will play a key role in promoting public health, including assessing sufficient and durable protection.

Kalen N. Olson, PhD, serves as Head of Medical Affairs and Medical Officer for Laboratory Diagnostics at Siemens Healthineers. Before joining Siemens Healthineers, she was the Clinical Laboratory Director at a large healthcare system in the Minneapolis/St. Paul metropolitan area.
Katherine Soreng, PhD, heads Global Clinical Education for Laboratory Diagnostics at Siemens Healthineers.
References
1. Walayat S, et al. Recent advances in vaccination of non-responders to standard dose hepatitis B virus vaccine. World J Hepatol. 2015 October 28;7(24):2503-9.
2. Stadlbauer D, et al. Repeated cross-sectional sero-monitoring of SARS-CoV-2 in New York City. Nature. 2020. https://doi.org/10.1038/s41586-020-2912-6
3. Dingens AS. Seroprevalence of SARS-CoV-2 among children visiting a hospital during the initial Seattle outbreak. Nature Communications. 2020. 11:4378. https://doi.org/10.1038/s41467-020-18178-1
4. Gudbjartsson DF, et al. Humoral immune response to SARS-CoV-2 in Iceland. N Engl J Med. 2020;383:1724-34. DOI: 10.1056/NEJMoa2026116
5. Alter G, Seder R. The power of antibody-based surveillance. N Engl J Med. 2020; 383:1782-4. DOI:10.1056/NEJMe2028079
6. Perico, L. et al. COVID-19 and Lombardy: TESTing the impact of the first wave of the pandemic. EBioMedicine. 2020. DOI: 10.1016/j.ebiom.2020.103069
7. https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antibody-tests-guidelines.html. Accessed November 6, 2020.
8. https://www.idsociety.org/COVID19guidelines/serology. Accessed November 6, 2020.
9. Rodda, L.B. et al. Functional SARS-CoV-2-specific immune memory persists after mild COVID-19. https://doi.org/10.1101/2020.08.11.20171843. This version posted August 15, 2020.
10. Piccoli L, et al. Mapping neutralizing and immunodominant sites on the SARS-CoV-2 spike receptor-binding domain by structure-guided high-resolution serology. Cell. 2020. https://doi.org/10.1016/j.cell.2020.09.037.
11. Premkumar, et al. The receptor binding domain of the viral spike protein is an immunodominant and highly specific target of antibodies in SARS-CoV-2 patients. 2020. Sci. Immunol. DOI: 10.1126/sciimmunol.abc8413.
12. Wang, H. et al. Development of an inactivated vaccine candidate, BBIBP-CorV, with potent protection against SARSCoV-2. 2020. Cell. 182;713-21.
13. Addetia, A., et al. Neutralizing antibodies correlate with protection from SARS-CoV-2 in humans during a fishery vessel outbreak with a high attack rate. 2020. J Clin Microbiol. 58:e02107-20. https://doi.org/10.1128/JCM.02107-20.
14. Corbett KS, et al. Evaluation of the mRNA-1273 vaccine against SARS-CoV-2 in nonhuman primates. N Engl J Med. 2020 Jul 28:NEJMoa2024671. doi: 10.1056/NEJMoa2024671.
15. Walsh, E.E. et al. Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine Candidates. N Engl J Med. 2020 383:2439-50. DOI: 10.1056/nejmoa2027906.
16. Mercado NB, et al. Single-shot Ad26 vaccine protects against SARS-CoV-2 in rhesus macaques. Nature. 2020. https://doi.org/10.1038/s41586-020-2607-z
17. Wajnberg A, et al. Robust neutralizing antibodies to SARS-CoV-2 infection persist for months. Science. 2020. DOI: 10.1126/science.abd7728.
18. Long, Q. et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections. Nat Med. 2020;26:1200-4. https://doi.org/10.1038/s41591-020-0965-6
19. Seow, J. et al. Longitudinal observation and decline of neutralizing antibody responses in the three months following SARS-CoV-2 infection in humans. Nat Microbiol. 2020. https://doi.org/10.1038/ s41564-020-00813-8
20. Muecksch F, et al. Longitudinal analysis of clinical serology assay performance and neutralising antibody levels in COVID19 convalescents. medRxiv. 2020.08.05.20169128. https://doi.org/10.1101/2020.08.05.20169128
21. Ripperger TJ, et al. Detection, prevalence, and duration of humoral responses to SARS-CoV-2 under conditions of limited population exposure. medRxiv. 2020.08.14.20174490; DOI: https://doi. org/10.1101/2020.08.14.20174490
22. Ibarrondo, F.J. et al., et al. Rapid decay of anti–SARS-CoV-2 antibodies in persons with mild Covid-19. N Engl J Med.2020;383:1085-7.
23. Wang Y, et al. Kinetics of viral load and antibody response in relation to COVID-19 severity. J Clin Invest. 2020;130(10):5235-44. https://doi.org/10.1172/JCI138759.
24. Grandjean L, et al. Humoral response dynamics following infection with SARS-CoV-2. medRxiv. 2020.07.16.20155663; https://doi.org/10.1101/2020.07.16.20155663
25. Fenwick, C. et al. Changes in SARS-CoV-2 antibody responses impact the estimates of infections in population-based seroprevalence studies. medRxiv 2020.07.14.20153536. https://doi.org/10.1101/2020.07.14.20153536
26. Harvala, H. et al. Convalescent plasma treatment for SARS-CoV-2 infection: analysis of the first 436 donors in England, 22 April to 12 May 2020. Euro Surveill. 2020;25(28):2001260. DOI:10.2807/1560- 7917.ES.2020.25.28.2001260
27. Poland GA, et al. SARS-CoV-2 immunity: review and applications to phase 3 vaccine candidates. Published online October 13, 2020. https://doi.org/10.1016/S0140-6736(20)32137-1
28. Erasmus JH, et al. An alphavirus-derived replicon RNA vaccine induces SARS-CoV-2 neutralizing antibody and T cell responses in mice and nonhuman primates. Sci Transl Med. 2020. DOI: 12(555):eabc9396.
29. Jeyanathan M, et al. Immunological considerations for COVID-19 vaccine strategies. Nat Rev Immunol. 2020;20:615-32. https://doi.org/10.1038/s41577-020-00434-6
30. Chen Y, et al. Aging in COVID-19: vulnerability, immunity and intervention. Ageing Res Rev. 2020 Oct 31:101205. DOI: 10.1016/j.arr.2020.101205
31. Poonia, B. and Kottilil, S. Immune correlates of COVID-19 control. Front Immunol. 2020;11:569611. DOI: 10.3389/fimmu.2020.569611
32. Chaplin DD. Overview of the immune response. J Allergy Clin Immunol. 2010 Feb;125(2 Suppl 2):S3-23. DOI: 10.1016/j. jaci.2009.12.980
33. Marshall, J.S. et al. An introduction to immunology and immunopathology. Allergy Asthma Clin Immunol. 2018 Sep 12;14(Suppl 2):49. DOI:10.1186/s13223-018-0278-1
34. Van Blargan LA, et al. Deconstructing the antiviral neutralizing- antibody response: implications for vaccine development and immunity. Microbiology and Molecular Biology Reviews. 2016 Oct; 80(4):989-1010. DOI: 10.1128/MMBR.00024-15
35. Chen X, et al. Disease severity dictates SARS-CoV-2-specific neutralizing antibody responses in COVID-19. Sig Transduct Target Ther. 2020;5:180. https://doi.org/10.1038/s41392-020-00301-9
36. Hassan AO, et al. A SARS-CoV-2 infection model in mice demonstrates protection by neutralizing antibodies. Cell. 2020 Aug 6;182:744-53. https://doi.org/10.1016/jcell.2020.06.011
37. Krammer F. SARS-CoV-2 vaccines in development. Nature. 2020;586:516-27. https://doi.org/10.1038/s41586- 020-2798-3
38. Iyer AS, et al. Persistence and decay of human antibody responses to the receptor binding domain of SARS-CoV- 2
spike protein in COVID-19 patients. Science Immunology.
2020 Oct 8;5(52):eabe0367. DOI: 10.1126/sciimmunol.abe0367
39. Iyer AS. Dynamics and significance of the antibody response to SARS-CoV-2. medRxiv. 2020.07.18.20155374. DOI:10.1101/2020.07.18.20155374
40. Figueiredo-Campos P, et al. Seroprevalence of anti-SARS-CoV-2 antibodies in COVID-19 patients and healthy volunteers up to 6 months post disease onset. Eur J Immunol. 2020;00:1-16. DOI: 10.1002/eji.202048970.
41. Isho B, et al. Persistence of serum and saliva antibody responses to SARS-CoV-2 spike antigens in COVID-19 patients. Sci Immunol. 2020;5(52):eabe5511. DOI: 10.1126/sciimmunol.abe5511
42. Xia, S. et al. Effect of an inactivated vaccine against SARS-CoV-2 on safety and immunogenicity outcomes: interim analysis of 2 randomized clinical trials. JAMA. DOI:10.1001/jama.2020.15543
43. Folegatti PM, et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: a preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet. 2020;396:467-78. https://doi.org/10.1016/S0140- 6736(20)31604-4
44. Zhu, F.C. et al. Safety, tolerability, and immunogenicity of a recombinant adenovirus type-5 vectored COVID-19 vaccine: a dose-escalation, open-label, non-randomised, first-in-human trial. Lancet. 2020;395:1845-54. https://doi.org/10.1016/S0140- 6736(20)31208-3
45. Zhu, F.C. et al. Immunogenicity and safety of a recombinant adenovirus type-5-vectored COVID-19 vaccine in healthy adults aged 18 years or older: a randomised, double-blind, placebo- controlled, phase 2 trial. Lancet. 2020;396(10249):479-88. DOI: https://doi.org/10.1016/S0140-6736(20)31605-6
46. Logunov DY, et al. Safety and immunogenicity of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine in two formulations: two open, non-randomised phase 1/2 studies from Russia. Lancet. 2020;396:887-97. https://doi.org/10.1016/S0140-6736(20)31866-3
47. Jackson LA, et al. An mRNA vaccine against SARS-CoV-2 — preliminary report. N Engl J Med. 2020 Jul 14;383:1920-31. DOI: 10.1056/NEJMoa2022483.
48. Keech C, et al. Phase 1–2 trial of a SARS-CoV-2 recombinant spike protein nanoparticle vaccine. DOI:10.1056/NEJMoa2026920
49. Zhang, Y.J. et al. Immunogenicity and safety of a SARS-CoV-2 inactivated vaccine in healthy adults aged 18-59 years: report of the randomized, double-blind, and placebo-controlled phase 2 clinical trial. medRxiv. 2020.07.31.20161216; https://doi.org/10.1101/2020.07.31.20161216
50. Hotez, P.J. et al. COVID-19 vaccines: neutralizing antibodies and the alum advantage. Nat Rev Immunol. 2020;20:399-400. https://doi.org/10.1038/s41577-020-0358-6
51. Dagotto G, et al. Approaches and challenges in SARS-CoV-2 vaccine development. Cell Host Microbe. 2020 Sep 9;28(3):364-70. Published online 2020 Aug 10. DOI: 10.1016/j.chom.2020.08.002
52. Yu J, et al. DNA vaccine protection against SARS-CoV-2 in rhesus macaques. Science. 2020 Aug 14;369(6505):806-11.
DOI: 10.1126/science.abc6284. Epub 2020 May 20.
53. van Doremalen N, et al. ChAdOx1 nCoV-19 vaccine prevents SARS-CoV-2 pneumonia in rhesus macaques. Nature. 2020;586:578-82. https://doi.org/10.1038/s41586-020-2608-y
54. Gao Q, et al. Development of an inactivated vaccine candidate for SARS-CoV-2. Science. 2020;369:77-81. DOI: 10.1126/science.abc1932.
55. Mulligan MJ, et al. Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature. 2020;586:589-93. https://doi.org/10.1038/s41586-020-2639-4
56. Sahin U, et al. COVID-19 vaccine BNT162b1 elicits human antibody and TH1 T cell responses. Nature. 2020;586:594-9. https://doi.org/10.1038/s41586-020-2814-7
57. Bos R, et al. Ad26 vector-based COVID-19 vaccine encoding a prefusion-stabilized SARS-CoV-2 spike immunogen induces potent humoral and cellular immune responses. NPJ Vaccines. 2020 Sep 28;5:91. DOI: 10.1038/s41541- 020-00243-x.
58. Bubar, K.M. et al. Model-informed COVID-19 vaccine prioritization strategies by age and serostatus. medRxiv 2020.09.08.20190629; https://doi.org/10.1101/2020.09.08.20190629
59. Gaebler, C. & Nussenzweig, M.C. All eyes on the hurdle race for a SARS-CoV-2 vaccine. Nature. 2020 Oct 22;586:501-2. https://www.nature.com/articles/d41586-020-02926-w
60. Trabaud, M.A. et al. Comparison of eight commercial, high- throughput, automated or ELISA assays detecting SARS-CoV-2 IgG or total antibody. Journal of Clinical Virology. 2020;132:104613. https://doi.org/10.1016/j.jcv.2020.104613
61. Houlihan, C.F. and Beale R. The complexities of SARS-CoV-2 serology. 2020 Sep 23. https://doi.org/10.1016/S1473- 3099(20)30699-X
62. National SARS-CoV-2 Serology Assay Evaluation Group. Performance characteristics of five immunoassays for SARS-CoV-2: a head-to-head benchmark comparison. Lancet Infect Dis. Published online 2020 Sep 23. DOI:10.1016/S1473- 3099(20)30634-4
63. Rosadas C, et al. Testing for responses to the wrong SARS-CoV-2 antigen? Lancet. 2020 Sep 5; 396(10252):E23. https://doi.org/10.1016/S0140-6736(20)31830-4.
64. https://www.fda.gov/medical-devices/coronavirus-disease- 2019-covid-19-emergency-use- authorizations-medical-devices/ eua-authorized-serology-test-performance.
Accessed November 12, 2020.
65. https://www.siemens-healthineers.com/press-room/press-releases/ covid-19-antibody-igg.html. Accessed November 12, 2020.
66. https://www.roche.com/media/releases/med-cor-2020-09-18b.htm. Accessed November 12, 2020.
67. https://newsnetwork.mayoclinic.org/discussion/mayo-clinic- launches-neutralizing-antibody-test-to- advance-covid-19- therapies/. Accessed November 12, 2020.
68. FDA. Development and licensure of vaccines to prevent COVID-19. Guidance for industry. https://www.fda.gov/media/139638/ download. Accessed November 8, 2020.
69. Corbett KS, et al. SARS-CoV-2 mRNA vaccine design enabled by prototype pathogen preparedness. Nature. 2020. https://doi.org/10.1038/s41586-020-2622-0



{kind=link}