
A broader screening approach may improve population-level control of sexually transmitted infections
By Barbara Van Der Pol, PhD, MPH
According to the most recent data from the US Centers for Disease Control and Prevention (CDC), sexually transmitted infections (STIs) in the United States are on the rise. One important reason for this rise is the underutilization of screening.
CDC recommends that all sexually active women under the age of 25 be screened annually. But the agency also estimates that only 12% of such individuals actually undergo testing. Clinicians generally acknowledge that the current approach of taking a sexual history during an office visit does not enable them to identify those who are truly at risk. Consequently, several recent studies have examined an alternative universal screening or ‘opt-out’ approach.
This article describes the current prevalence of bacterial STIs in the United States, the development and limitations of current screening practices, and what it would mean for patients and clinical laboratories if healthcare providers adopted a universal screening strategy for STIs.
Controlling Treatable STIs
Chlamydia trachomatis and Neisseria gonorrhoeae are the two most common notifiable infectious diseases in the United States, with nearly 1.6 million new cases of chlamydial infection and 0.5 million incident gonococcal infections reported in 2016—and rates continuing to rise.1
To contextualize these numbers, the third most commonly reported infectious disease is salmonellosis, only 55,000 cases of which were reported in 2015.2
In many populations Trichomonas vaginalis is more common than chlamydia and gonorrhea combined, with an estimate of more than 3.5 million cases treated per year.3 However, T. vaginalis is not a notifiable infection and, as a result, the estimates of case rates and prevalence are much less precise for T. vaginalis infection than for either chlamydia or gonorrhea.
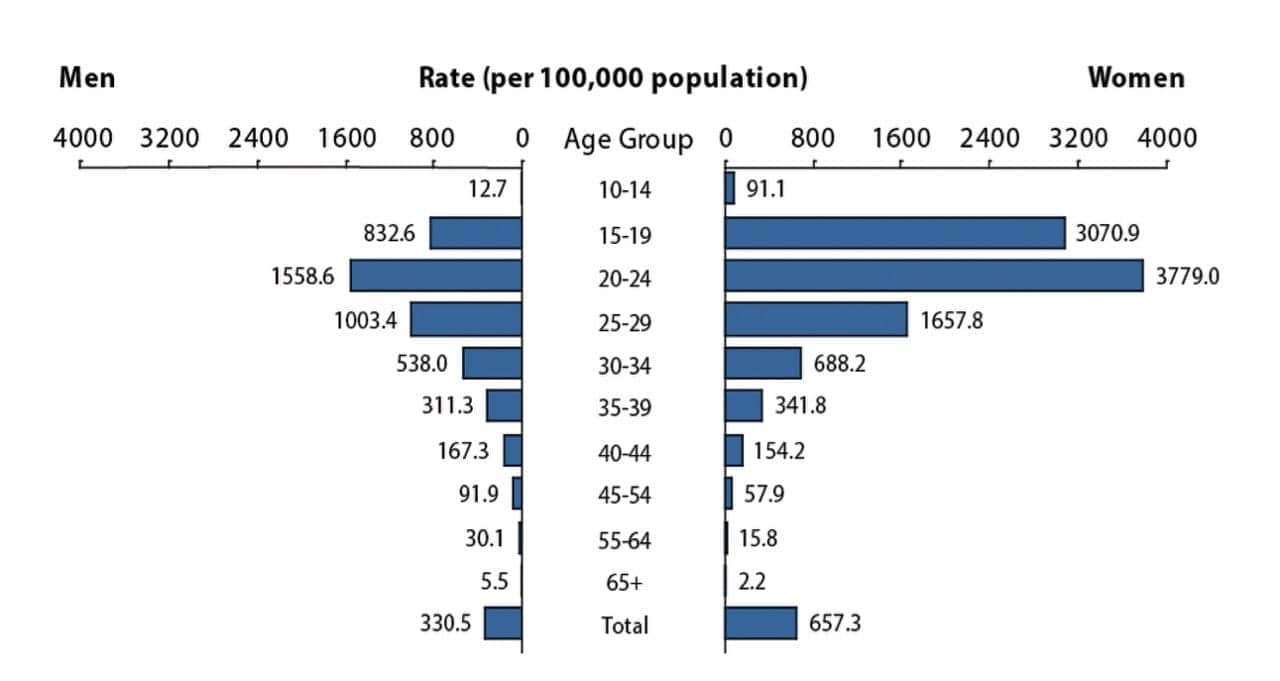
Figure 1. The distribution of reported chlamydial infections in the United States by age and sex, 2016.1
Despite requirements that healthcare providers report identified chlamydia and gonorrhea infections, the passive surveillance system used in the United States very clearly underestimates the true burden of these diseases, for a number of reasons. First, there is hesitancy on the part of practitioners to report this information to local and state agencies due to concerns about client privacy, embarrassment, and stigma. Second, only those cases that are detected can be reported and thus, since many individuals are not screened when they access the healthcare system, unidentified cases cannot be reported. And third, there is a significant proportion of cases not identified due to a lack of access to services, whether due to location (eg, rural populations) or healthcare coverage status (eg, economically disadvantaged populations). For all of these reasons, the true number of STIs occurring each year in the United States is unknown. Best estimates are in the range of 3 million to 5 million cases of chlamydia, 0.7 million to 1.5 million cases of gonorrhea, and 7 million cases of trichomonas.
Left untreated, these STIs have each been associated with significant downstream health consequences, mostly borne by women. C. trachomatis infections have been well established as leading to the development of pelvic inflammatory disease (PID), ectopic pregnancy, tubal factor infertility, and the potential for neonatal complications.4,5
N. gonorrhoeae has also been associated with PID, neonatal complications, and increased risk of acquisition of HIV.4 Further, N. gonorrhoeae has the capacity to develop resistance to antimicrobials.6,7 Finding and treating cases before resistance to available treatment regimens develops is of substantial importance to public health management of this infectious disease.
T. vaginalis has been associated with adverse outcomes of pregnancy, and increased risk of both acquisition and transmission of HIV.8–11 Given the high prevalence of trichomonas infections among groups at high risk for HIV, this is a serious concern both globally and in the United States.
The annual cost of the sequelae of untreated infections with chlamydia, gonorrhea, or trichomonas is estimated to be approximately $600 million, but may be closer to $1 billion in today’s dollars.12 These estimates do not include costs associated with STI-induced infertility or HIV. Preventing such downstream consequences and associated costs through effective screening and early treatment is the goal of all sexually transmitted disease (STD) prevention programs.
The Current Paradigm
Recommendations for population screening to detect chlamydia infections have been in place for more than two decades. The organizations responsible for such recommendations encompass several prominent government agencies and nationally recognized authorities, including CDC, the US Preventive Services Task Force (USPSTF), and the National Committee for Quality Assurance—the organization that generates the health effectiveness data and information set (HEDIS) measures used to assess the quality of provider services.5,13,14 Each of these organizations recommends screening of all sexually active women under the age of 25, men and women in high-prevalence settings or populations, and those who engage in sexual behaviors that could put them at risk for STIs.
Despite the existence of such guidelines, the rates of chlamydia infection continue to increase, due in part to payors’ unwillingness to offer reimbursement coverage for broad-based population screening. HEDIS data through 2016 suggest that less than 55% of women using Medicaid, and less than 43% of women with commercial third-party insurance, were actually screened as recommended.15 Coverage is even lower among women aged 15 to 19, for whom the risk of infection is actually greatest (Figure 1). Such gaps in screening coverage raise concerns about the capacity of the US healthcare system to provide effective STI screening services capable of substantially slowing the growing prevalence of these diseases.
The changing landscape of healthcare services in the United States may further reduce the ability of the healthcare system to achieve the goal of screening at-risk individuals on an annual basis. Throughout the country, federally funded STD clinics are being shut down, and clinics that once routinely provided reproductive healthcare to those with no other source of medical care are dealing with substantial funding cuts. As a result, women are now seeking these services in general practice settings more than in the past.
Information about who reports identified infections can serve as a surrogate for understanding where testing is being performed (Figure 2). According to CDC data, it is clear that men are receiving services at non-STD clinic settings much more frequently than in the past. But it is much less clear where women are receiving such services. Such unpredictability suggests that healthcare providers working in any setting should be prepared to provide screening services for women in the appropriate age range who have not been tested within the past year.
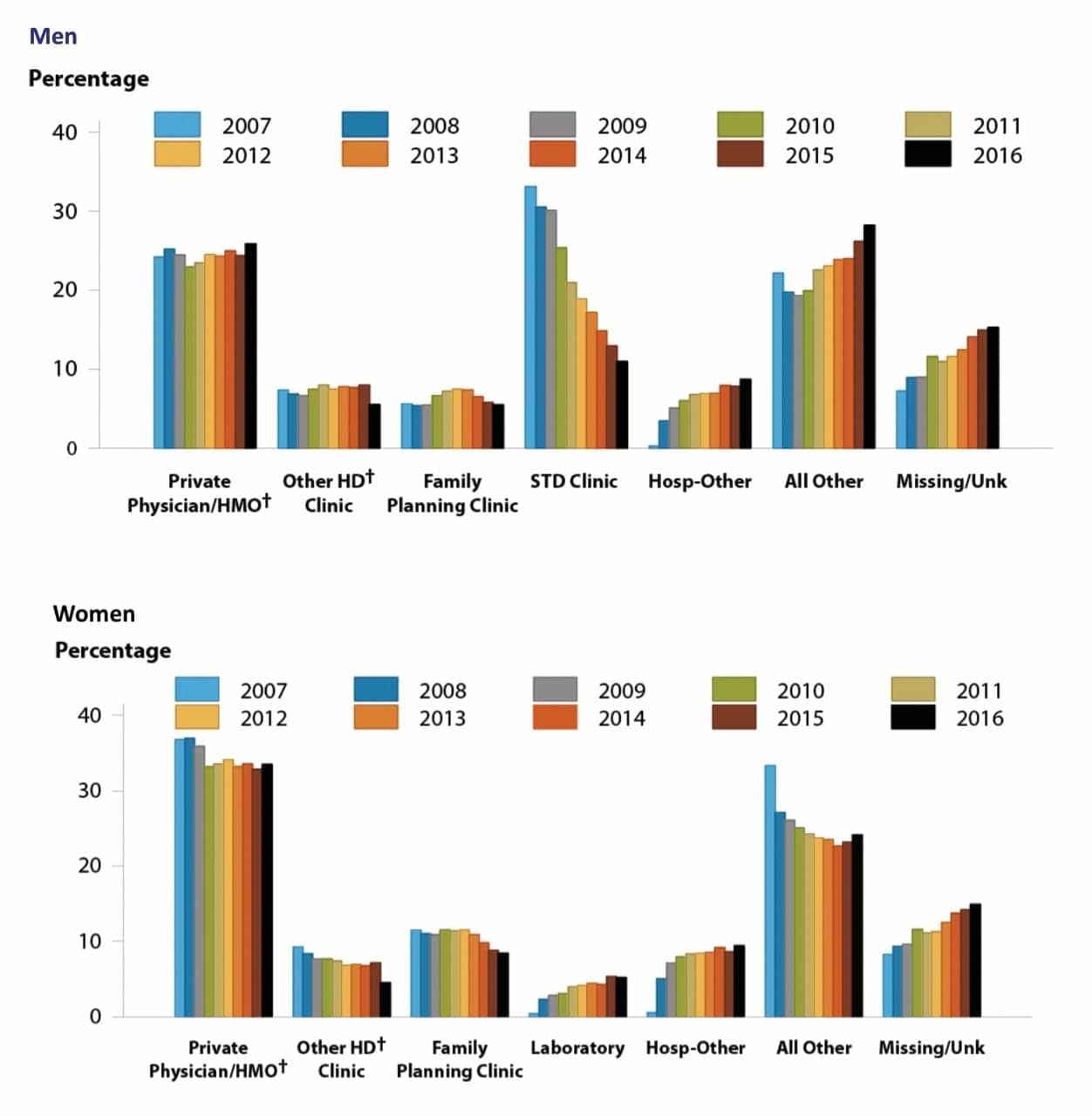
Figure 2. Changes in the provision of sexually transmitted infection screening in the United States, by reporting source, 2007–2016. HD = health department. HMO = health maintenance organization. Adapted from the Centers for Disease Control and Prevention.1
Making STI testing available in virtually any clinical setting has been greatly facilitated by the common availability of nucleic acid amplification tests. CDC has recommended that both screening of asymptomatic patients and diagnostic testing should be performed using nucleic acid amplification tests.16 Such molecular laboratory methods are a significant improvement over any other technology currently available and provide significantly improved case findings over older methods.
Nucleic acid amplification tests have been widely adopted for the detection of chlamydia and gonorrhea. But uptake of molecular testing for trichomonas has lagged, in spite of excellent data demonstrating that diagnosis by microscopy or clinical symptoms lacks sensitivity.17 Since molecular testing for T. vaginalis is now widely available as an add-on to chlamydia/gonorrhea testing (using the same specimen), it is critical to the improvement of case findings that clinicians request this testing.18,19
The development and availability of nucleic acid amplification tests for STIs is an instance where technology developers have already provided the solutions necessary to meet the needs of clinicians and their patients, but the culture of healthcare services has not kept pace with the available advances in laboratory medicine. Study data have repeatedly demonstrated that improved adherence to screening recommendations would result in substantial reductions in risks to individuals’ sexual and reproductive health, as well as substantial healthcare savings. But realizing such benefits will require healthcare providers to improve screening practices by implementing solutions that take advantage of advanced technologies.
Barriers against STI Control Efforts
Diagnosis and treatment of STIs can prevent individuals’ future health complications, and can also reduce the burden of such diseases in the overall population. But a major barrier to the widespread achievement of such a goal is the fact that a substantial proportion of STIs produce no obvious symptoms, so diagnostic testing may never be requested or performed.
For STI testing to be truly impactful, it is essential that the tests be performed for screening—testing in the absence of overt symptoms—in populations shown to have above average prevalence of STIs. To determine the level of prevalence at which such screening should be performed, clinicians can use data generated by the National Health and Nutrition Examination Survey (NHANES), a nationally representative population from which samples are collected for STI surveillance.
NHANES data through 2012 estimates that the overall prevalence of chlamydia in the United States among women aged 14 to 39 is 1.7%. However, the prevalence of chlamydia among the subset of women aged 14 to 24 is 4.7%, and the prevalence among non-Hispanic black women of the same age is 13.5%.20 The substantially higher prevalence of chlamydia among young women is part of the rationale for screening recommendations targeted at women under the age of 25.
However, women under age 30 also have a substantial burden of STIs. And for men under age 30—for whom there are no broad screening recommendations—the prevalence of STIs remains substantial. Among men, age-specific prevalence is shifted in favor of a slightly higher age group than for women (Figure 1).
Improving the Effectiveness of Current Recommendations
Several strategies have been proposed to increase providers’ willingness to offer screening, patients’ utilization of such services when offered, and individuals’ access to screening services. Proposed strategies include:
- Providing pre- and postexposure prophylaxis.
- Incentivizing patients to provide samples for annual screening.
- Recommending a universal testing and opt-out strategy among populations known to have high rates of disease.
- Offering screening services in nonclinical settings.
- Offering sample collection at home with Internet-based test requesting.21
Many such programs have been implemented as research or demonstration projects, resulting in the generation of data that allow mathematical modeling to predict the long-term effects of the strategies.
With any innovation intended to improve STI control efforts, thoughtful consideration is required to avoid unanticipated consequences. For example, pre- and postexposure prophylaxis has been a successful tool in the effort to control HIV, and has been proposed as a strategy for reducing the prevalence of syphilis in the United States. However, in light of global concern for antimicrobial stewardship in general, and specific concerns related to the rise of antibiotic-resistant N. gonorrhoeae organisms, antibiotic prophylaxis on a significant scale is unlikely to be a sound strategy.
Similarly, while research projects have shown that paying individuals to utilize services may help to bring in patients who are not currently using the services, translating such research activities into sustainable programs has been difficult.22 Such difficulties should not be surprising in light of the limited resources available to public health authorities and the dearth of private payor reimbursement for all testing costs—much less for this type of client incentivization. In private practice, the payment of such incentives is simply not economically feasible. And in public health settings, implementing such a program would require authorities to choose between paying for lab tests or paying for clients (and thus being able to afford fewer tests overall). Further, it has proven to be very challenging to reach those who should be participating and to manage incentivization.
A promising strategy now being discussed would eliminate targeted screening for women—a model that requires providers to take a full sexual history and make risk-based decisions about testing and treatment—and would implement universal screening, with an opt-out option, among those in populations with high rates of disease.23,24 Because no clinical population is truly homogenous, defining levels that constitute a ‘high rate’ should likely depend on data for regional populations rather than for clinic-specific populations.
Implementation of such a universal screening strategy would apply to both women and men in appropriate age brackets. Current recommendations for men focus only on those with symptoms suggestive of an STI or those who report sexual behaviors that may increase the risk of infection. But such testing recommendations have not resulted in substantial increases in screening volume among men, nor any reductions in disease prevalence in such high-burden regions as the US Deep South (Figure 1). The most appropriate methods for identifying more individuals with asymptomatic infections would be either to collect a detailed sexual history that would guide targeted screening, or simply to screen all individuals in the appropriate age range who have not had a negative test within the past year.
Such a universal screening approach, with opt-out, for men and women who have no record of a negative test within the past year and who are in high-prevalence settings and age groups, may result in improved control efforts compared to the current paradigm.
A recent study of universal opt-out screening suggests that implementation of such a model may provide an improved process for identifying STIs.25 According to this study, universal opt-out testing of those already engaged with the healthcare system would realize both a reduction in downstream health sequelae and a savings in costs—despite the increased number of tests being performed. The models evaluated in the study did not include infertility-related costs, HIV acquisition, or the effects of increasing rates of antimicrobial-resistant strains of N. gonorrhoeae.7 When considering these additional and expensive outcomes that could be avoided, the savings associated with universal opt-out screening could be even more substantial.
Implementation of Universal Screening
Healthcare providers play an important role in the delivery of sexual health services to their patients. However, providers also perceive a number of major barriers that limit their ability to provide such services, including the time and comfort level required to obtain a patient history sufficient to assess sexual risk, the time needed to educate patients about STIs, and the time needed to collect appropriate specimens.26,27
Such barriers can be addressed by shifting STI screening to a routine and simplified clinical process that reduces the stigma and time requirements associated with STI tests. Many women seek sexual and reproductive healthcare services from obstetrics and gynecology specialists or family planning clinics on an annual basis, in part to receive Pap testing for cervical cancer screening. As the guidelines for cervical cancer screening are evolving, however, it is possible that such testing may soon no longer be reimbursable on an annual basis. Consequently, now is the time to take advantage of the routine healthcare-seeking behavior that already exists among women patients, by shifting the focus of annual checkups to sexual health screening, while such annual screening is currently normative.
Routine screening of all clients in the appropriate age range would encourage a sexual health approach, rather than a disease-finding approach, since the vast majority of clients will have no infections. Nevertheless, adopting such a universal screening strategy would improve the ability of clinicians to identify asymptomatic infections. Such a positively framed approach to sexual healthcare could have the added benefit of improving the ability of both clients and practitioners to engage in frank conversations about potential sexual exposures and risks, thus improving the ability of each to gain information important to sexual healthcare management.
Clinical workflow solutions have the potential to encourage the provision and utilization of routine sexual healthcare services. In many clinics that offer sexual and reproductive health services, the normal workflow routes women to provide a urine sample immediately upon their arrival. Asking women to obtain a self-collected vaginal swab at the same time would be an obvious time-saver. Further, making such sample collection normative would reduce the stigma associated with being asked to provide a sample for STI screening. Given the limited time that clinicians have to speak with their patients, and the discomfort that many feel when asking about sexual risk behaviors, making STI sample collection normative would be an efficient workflow solution that encourages screening.

Figure 3. The Panther automated testing platform by Hologic, Marlborough, Mass, offers a broad menu of FDA-cleared or -approved assays for sexually transmitted infections, women’s health, and virology.
Examples of such normative sample collection include blood draws used to screen pregnant women for syphilis. Most women do not know why their blood is being drawn or what tests are being performed—and most never have a need to find out. Without encouraging any intentional lack of transparency, similarly normative collection of samples from all women would be an important step toward making STI testing a routine part of an annual healthcare visit. Gaining experience with reporting results that are most often negative may also encourage healthcare providers to begin engaging in conversations about sexual health without feeling as if they are always the bearers of bad news.
Finally, and in certain cases most importantly, identification of asymptomatic infections will offer healthcare providers the opportunity to assess their patients for other STIs. For instance, Mycoplasma genitaliumis often found as a coinfection with other well-recognized STIs, and current data suggest that such infections may play a role in the development of PID and adverse pregnancy outcomes.28 Coinfection with syphilis or with herpes simplex virus is also frequently encountered among patients with other STIs.
When patients return for treatment of an identified infection, healthcare providers will have an easy opportunity to perform a more-thorough examination than would have been warranted for an asymptomatic patient, and to identify other manageable conditions. Patients with positive results should be rescreened within the following 3 to 6 months; this repeat testing is also less stigmatized when it is performed in a clinic where all patients routinely collect samples for STI screening.
The Laboratory’s Role
Laboratory and clinical services are often perceived as being at opposite ends of the healthcare spectrum. In reality, however, the relationship is very integrated, with each group influencing the other. This continuous feedback process is exemplified by the history of chlamydia diagnostics.
When C. trachomatis was initially classified as an STI, the only diagnostic option was recovery of viable organisms using tissue culture methods performed in specialized laboratories. The process required adequate sample collection, cold-chain transport, immediate processing in the laboratory (within 24 hours), and very specialized laboratory equipment and skillsets. Thus, access to testing services was generally available only in urban centers with the capabilities of larger reference or research laboratories. As clinical demand for broader access to diagnostics increased, non-culture methods were developed. C. trachomatis was one of the first pathogens to be targeted by molecular diagnostics because of the need to detect nonviable organisms in low copy numbers (Figure 3).
With the availability of nucleic acid amplification tests, it became possible to use new specimen types (eg, vaginal swabs and urine specimens) that could be readily captured through patient self-collection. The application of molecular diagnostics brought about disruptive changes by facilitating the screening of asymptomatic patients in settings that lacked the capacity to perform pelvic exams or collect urethral swabs, and by eliminating the need to send samples to reference laboratories for testing. Instead, screening could be performed in fast-track clinics (where patients are triaged to self-collection of samples coupled with nothing more than a blood draw), school health clinics, detention centers, workforce entry screening clinics, and community-based outreach events with limited or no clinical facilities.
This single advance in laboratory medicine increased the capacity and reach of STI control programs by an order of magnitude. Thus, we have a very clear example of clinical need providing the impetus for laboratory advances, followed by improved laboratory technologies affecting the provision of healthcare services in both clinical and nonclinical settings.
Laboratories are critical to the conversation about screening efficiencies, which in turn plays an important role in calculating the costs of testing. With the implementation of a universal opt-out approach to screening, laboratories will have increased sample volumes and will benefit from the adoption of testing methods capable of detecting multiple pathogens in a single sample, with throughput appropriate for the expected testing volume (Figure 4).
As screening becomes a routine element of individuals’ sexual healthcare practices, laboratories may begin to see an increase in consumer-based testing options, such as the home-collection kits that are currently being sold in large retail stores and online. Laboratories will need to be prepared to support the services requested via this patient-driven healthcare option. To meet the needs of all their clients, laboratories will need to be prepared to offer a broad menu of tests, and to handle the resulting increase in test volumes.
Laboratories will remain important for improving understanding of current testing practices as well as for developing the next generation of tools that will change future healthcare services for STIs. Laboratories typically maintain large repositories of undisseminated data, including the number of patients tested, number of tests performed, and positivity rates. To generate case rates by region, the healthcare community currently relies on laboratory reporting of notifiable diseases, but these calculations are based on use of the overall population census as the denominator.
Figure 4. The Aptima Combo 2 test by Hologic, Marlborough, Mass, detects rRNA from Chlamydia trachomatis and Neisseria gonorrhoeae.
By contrast, laboratories typically have much more complete data reflecting real denominators—the numbers of patients they have actually served and the number of tests they have actually performed. When shared publicly through outcomes and epidemiologic research, such data can effectively inform local and regional practice by establishing with greater certainty the relevant disease burden and service utilization information. For example, while CDC-generated positivity rates per 100,000 may indicate a low prevalence rate in a specific population, actual laboratory data showing that only a small subset of the population has ever been tested could lead to an understanding that the real prevalence rate is much higher.
In addition to their contributions to outcomes and population-level research, laboratories are usually on the front line in developing new assays to detect pathogens of emerging importance and in evaluating new strategies that facilitate testing. In the absence of FDA-cleared assays for the detection of T. vaginalis and M. genitalium, for instance, laboratories led the way by creating laboratory-developed tests for these pathogens. T. vaginalisis now included as an analyte on most systems that have assays for chlamydia and gonorrhea, and M. genitalium assays are currently under evaluation in the United States on several diagnostic platforms.
To facilitate the collection of STI specimens in a variety of settings and populations, laboratories took the lead in validating the use of vaginal swabs—and later, the use of anorectal and oropharyngeal samples—for the detection of chlamydia and gonorrhea. Public health agencies subsequently used the data generated by laboratory research to make recommendations about the importance of these sample types. And in turn, assay manufacturers have relied on such data and recommendations when conducting studies in support of broadened sample-type claims for their assays.
Thus, laboratories play a number of key roles in improving efforts to control STIs. Laboratories anticipate increased test volume and devise methods for accommodating such increases; they investigate and develop methods to maintain cost efficiencies; and they disseminate important data generated through both research efforts and routine testing.
Conclusion
Clearly the current strategy of STI control is not having the desired impact in either the United States or other parts of the world. To curtail further increases in the prevalence of STIs, the healthcare community must take advantage of the tools supplied by diagnostic laboratories and test manufacturers to bring about changes in STI screening practices.
Accomplishing this goal will require the engagement of public health agencies, healthcare professionals, and laboratory scientists in both research and program planning designed to identify and evaluate novel strategies for STI control. By implementing such new approaches to STI screening, healthcare providers will improve their likelihood of achieving screening goals and reducing the burden of STIs on both individuals and the healthcare system as a whole.
Implementation of universal opt-out screening for populations experiencing high STI rates will likely require a variety of supporting mechanisms. For instance, engagement with clinical care providers will be necessary to demonstrate the advantages of routine screening in their practice settings. Similarly, to ascertain and demonstrate the effectiveness of universal screening, there will be a need to gather accurate data on the number of clients tested, number of tests performed, number of STI cases identified, and accurate costs. Obtaining a comprehensive picture of the process will be easiest if clinical and laboratory groups work together to merge the data they have on hand.
Clinical organizations that adopt universal opt-out STI screening as a normative clinical routine should be encouraged to share their experience through publication of the data they collect before, during, and following implementation of this change. Such information will encourage others to follow a successful blueprint for operationalization of this effort in other settings.
Beyond clinical organizations, community-based organizations that provide services to marginalized populations also need support and encouragement to consider adding STI screening to their menu of services. A number of such organizations—including HIV prevention outreach groups, providers of HIV pre- and postexposure prophylaxis services, and syringe exchange programs—have already undertaken STI screening efforts. The diagnostic tools available today allow and should encourage such outreach, which will help to make STI screening accepted as a routine part of any health promotion activity.
Finally, all available data regarding implementation of the universal opt-out strategy should be shared with public health agencies for their consideration when developing future STI control recommendations. Such recommendations are critical to securing public health funding, but they are also important for informing decisions about what testing practices should be reimbursed by both public and private healthcare systems.
As a result of improved technologies, the clinical laboratory community has opportunities to improve STI control that have never existed in the past. Laboratorians should mobilize now to take advantage of these opportunities to reduce the burden of STI in the United States.
Barbara Van Der Pol, PhD, MPH, is director of the sexually transmitted diseases laboratory at the University of Alabama. For further information contact CLP chief editor Steve Halasey via [email protected].
References
- Sexually Transmitted Disease Surveillance 2016. Atlanta: Centers for Disease Control and Prevention, 2017. Available at: www.cdc.gov/std/stats16/default.htm. Accessed May 18, 2018.
- Adams DA, Thomas KR, Jajosky RA, et al. Summary of notifiable infectious diseases and conditions—United States, 2015. MMWRMorb Mortal Wkly Rep. 2017;64(53):1–143; doi: 10.15585/mmwr.mm6453a1.
- Satterwhite CL, Torrone E, Meites E, et al. Sexually transmitted infections among US women and men: prevalence and incidence estimates, 2008. Sex Transm Dis. 2013;40(3):187?193; doi: 10.1097/OLQ.0b013e318286bb53.
- Soper DE. Pelvic inflammatory disease. Obstet Gynecol. 2010;116(2 Pt 1):419?428; doi: 10.1097/AOG.0b013e3181e92c54.
- Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR-03):1?137. Available at: www.cdc.gov/mmwr/preview/mmwrhtml/rr6403a1.htm. Accessed May 22, 2018.
- Wi T, Lahra MM, Ndowa F, et al. Antimicrobial resistance in Neisseria gonorrhoeae: global surveillance and a call for international collaborative action. PLoS Med. 2017;14(7):e1002344; doi: 10.1371/journal.pmed.1002344.
- Chesson HW, Kirkcaldy RD, Gift TL, Owusu-Edusei K Jr, Weinstock HS. An illustration of the potential health and economic benefits of combating antibiotic-resistant gonorrhea. Sex Transm Dis. 2018;45(4):250?253; doi: 10.1097/OLQ.0000000000000725.
- Kissinger P. Epidemiology and treatment of trichomoniasis. Curr Infect Dis Rep. 2015;17(6):1?9; doi: 10.1007/s11908-015-0484-7.
- Silver BJ, Guy RJ, Kaldor JM, Jamil MS, Rumbold AR. Trichomonas vaginalis as a cause of perinatal morbidity: a systematic review and meta-analysis. Sex Transm Dis. 2014;41(6):369?376; doi: 10.1097/OLQ.0000000000000134.
- Kissinger P, Amedee A, Clark RA, et al. Trichomonas vaginalis treatment reduces vaginal HIV-1 shedding. Sex Transm Dis. 2009;36(1):11?16; doi: 10.1097/OLQ.0b013e318186decf.
- Van Der Pol B, Kwok C, Pierre-Louis B, et al. Trichomonas vaginalis infection and human immunodeficiency virus acquisition in African women. J Infect Dis. 2008;197(4):548?554; doi: 10.1086/526496.
- Owusu-Edusei KJ, Chesson HW, Gift TL, et al. The estimated direct medical cost of selected sexually transmitted infections in the United States, 2008. Sex Transm Dis. 2013;40(3):197?201; doi: 10.1097/OLQ.0b013e318285c6d2.
- LeFevre ML. Screening for chlamydia and gonorrhea: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;161(12):902?910; doi: 10.7326/M14-1981.
- Khosropour CM, Broad JM, Scholes D, Saint-Johnson J, Manhart LE, Golden MR. Estimating chlamydia screening coverage: a comparison of self-report and healthcare effectiveness data and information set measures. Sex Transm Dis. 2014;41(11):665?670; doi: 10.1097/OLQ.0000000000000186.
- Chlamydia screening in women. Washington, DC: National Committee for Quality Assurance, 2017. Available at: www.ncqa.org/report-cards/health-plans/state-of-health-care-quality/2017-table-of-contents/chlamydia-screening. Accessed May 22, 2018.
- Papp J, Schachter J, Gaydos C, Van Der Pol B. Recommendations for the laboratory-based detection of Chlamydia trachomatis and Neisseria gonorrhoeae, 2014. MMWR Recomm Rep. 2014;63(RR-2):1?24. Available at:www.cdc.gov/std/laboratory/2014labrec/2014-lab-rec.pdf. Accessed May 21, 2018.
- Van Der Pol B, Kraft CS, Williams JA. Use of an adaptation of a commercially available PCR assay aimed at diagnosis of chlamydia and gonorrhea to detect Trichomonas vaginalis in urogenital specimens. J Clin Microbiol. 2006;44(2):366?373; doi: 10.1128/JCM.44.2.366-373.2006.
- Roth AM, Williams JA, Ly R, et al. Changing sexually transmitted infection screening protocol will result in improved case finding for Trichomonas vaginalis among high-risk female populations. Sex Transm Dis. 2011;38(5):398?400; doi: 10.1097/OLQ.0b013e318203e3ce.
- Schwebke J, Merriweather A, Massingale S, Scisney M, Hill C, Getman D. Screening for Trichomonas vaginalis in a large high-risk population: prevalence among men and women determined by nucleic acid amplification testing. Sex Transm Dis. 2018;45(5):e23?e24;doi: 10.1097/OLQ.0000000000000757.
- Torrone E, Papp J, Weinstock H. Prevalence of Chlamydia trachomatis genital infection among persons aged 14–39 years—United States, 2007–2012. MMWR Morb Mortal Wkly Rep. 2014;63(38):834?838. PMID: 25254560.
- Grennan T, Gilbert M, Hull M. A new avenue to explore in STI prevention. BCMJ. 2017;59(9):480–486. Available at: www.bcmj.org/bc-centre-disease-control/new-avenue-explore-sti-prevention. Accessed May 21, 2018.
- Lee R, Cui RR, Muessig KE, Thirumurthy H, Tucker JD. Incentivizing HIV/STI testing: a systematic review of the literature. AIDS Behav. 2014;18(5):905?912;doi: 10.1007/s10461-013-0588-8.
- Ditkowsky J, Shah KH, Hammerschlag MR, Kohlhoff S, Smith-Norowitz TA. Cost-benefit analysis of Chlamydia trachomatis screening in pregnant women in a high burden setting in the United States. BMC Infect Dis. 2017;17(1):155;doi: 10.1186/s12879-017-2248-5.
- Hull S, Kelley S, Clarke JL. Sexually transmitted infections: compelling case for an improved screening strategy. Popul Health Manag. 2017;20(S1):S1?S11. PMID: 28920768.
- Owusu-Edusei K Jr, Hoover KW, Gift TL. Cost-effectiveness of opt-out chlamydia testing for high-risk young women in the US. Am J Prev Med. 2016;51(2):216?224; doi: 10.1016/j.amepre.2016.01.007.
- Jozkowski KN, Geshnizjani A, Middlestadt SE. University health center providers’ beliefs about discussing and recommending sexual health prevention to women college students. Health Educator. 2013;45(1):22?30. Available at: https://files.eric.ed.gov/fulltext/EJ1014967.pdf. Accessed May 22, 2018.
- Khan A, Plummer D, Hussain R, Minichiello V. Does physician bias affect the quality of care they deliver? evidence in the care of sexually transmitted infections. Sex Transm Infect. 2008;84(2):150?151; doi: 10.1136/sti.2007.028050.
- Lis R, Rowhani-Rahbar A, Manhart LE. Mycoplasma genitalium infection and female reproductive tract disease: a meta-analysis. Clin Infect Dis. 2015;61(3):418?426; doi: d0.1093/cid/civ312.



{kind=link}