
By Julie MacKenzie, MBA; Reem Kassab, MLS (ASCP); and George Hong, PhD

Julie MacKenzie, MBA, Advanced Instruments.
When we think about cerebrospinal fluid (CSF) analysis, it helps to first step back for a historical overview. CSF was first described in the 1700s by several scientists, including Emanuel Swedenborg, Albrecht von Haller, Francois Magendie, and Thomas Willis.1 And later, in the late 1800s, Heinrich Quincke showed the ability to access CSF and popularized collection of the fluid through lumbar puncture. He also advocated that CSF be used for diagnostic purposes.1 The continual discussions of CSF and using it to aid diagnosis over three centuries attests that the fluid is indeed a precious clinical specimen.
In this article, we will walk through the importance of CSF, touch on the approaches to count cells in CSF, explore current practices, and raise some questions as we think about the future of CSF testing.
Clinical Importance of CSF
CSF is normally a clear, colorless fluid that bathes the brain and spinal cord. The fluid is formed primarily by secretions from the choroid plexus into the ventricles of the brain and, to a lesser extent, by excretions from ependymal cells. It contains glucose, electrolytes, amino acids, and other small molecules found in plasma, but has very little protein and few cells. CSF protects the central nervous system from injury, cushions it from the surrounding bone structure, provides it with nutrients, and removes waste products by returning them to the blood.2

Reem Kassab, MLS (ASCP), Advanced Instruments.
The indications for collecting CSF include four major categories of disease: central nervous system malignancy, demyelinating disease, meningeal infection, and subarachnoid hemorrhage.3
Most commonly, CSF is collected by lumbar puncture. In some cases, lateral cervical puncture, ventricular puncture, or cisternal puncture may be utilized.3 Typically, CSF is collected into three to four sterile tubes, without anticoagulant. Generally, the first tube is used for chemical or serological analysis, the second tube for microbial testing, and the third tube for cell count and differential. The fourth tube may be utilized for cytology or other specialized testing.3
Cell counts are performed as soon as possible after collection due to the instability of cellular constituents. Delayed testing can cause inaccurate results.4
CSF is normally clear and colorless. Abnormal CSF may appear cloudy, turbid, bloody, viscous, or clotted. Increased white blood cells (WBCs) in the CSF may be indicative of meningitis, malignancy, or demyelinating disease. For example, high white cell counts of neutrophils may indicate that the patient has a bacterial infection. And high white cell counts of lymphocytes may indicate that the patient has a viral infection such as tuberculosis, a fungal infection, or a cancer recurrence in the central nervous system. Normal ranges for WBCs are shown in Table 1.2,3

Table 1. Normal ranges for white blood cells (WBCs) and red blood cells (RBCs) in cerebrospinal fluid. Click to expand.
It is commonly accepted that red blood cells (RBCs) should not be present in normal CSF. RBCs in the CSF may be indicative of hemorrhage or the result of a traumatic lumbar puncture.5 A significant decrease in color between the first and last collection tubes is the first indication that RBCs in CSF may be due to a traumatic tap. In the case of a hemorrhage, all tubes are likely to be the same color. Depending on the laboratory procedure, a secondary visual assessment may be conducted of the CSF supernatant following centrifugation. A clear and colorless supernatant indicates a traumatic tap, while a xanthochromic supernatant reveals a hemorrhage.5 For most labs, a cell count comparison between the first and last tubes is performed to definitively conclude whether a traumatic tap or hemorrhage has occurred. Diagnostic range guidelines for CSF are shown in Table 2.6
Cell Counting Technologies

Table 2. Diagnostic range guidelines for CSF. Figures given for pressure, cell counts, and protein are approximations; exceptions are common. Click to expand.
Both manual and automated methods are used for evaluation of CSF (see Figure 1). The manual hemocytometer method is the gold standard for enumerating RBCs and total nucleated cells (TNCs). This method employs light microscopy and a glass or plastic counting chamber with an etched grid. Phase-contrast or stains, such as gentian violet, may be utilized to enhance cell recognition.3
Optical, impedance, and imaging technologies are the basic principles applied in automated cell counting. Flow cytometry is used in these methods. In flow cytometry, fluorescently labeled cells are excited by a light source as they pass through a flow cell in single file (hydrodynamic focusing). Photodetectors measure the light emitted by the cells using specific optical filters. Cells are then categorized on the basis of size, granularity, and nucleic acid content.7,8
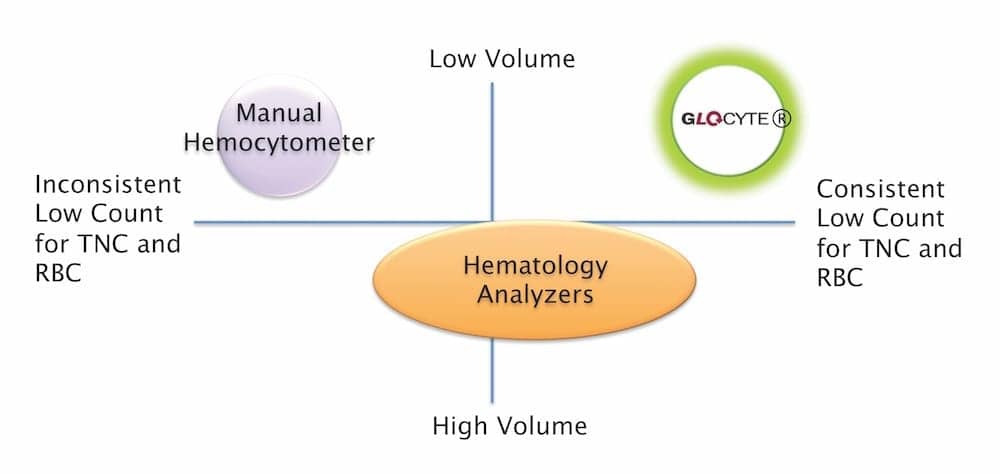
Figure 1. Comparison of CSF cell count methods. Click to expand.
With impedance technology, cells are sized and counted by detecting and measuring changes in electrical resistance as they pass through a small aperture. Two electrodes establish an electrical current. Resistance to the current occurs as the cells pass through the aperture. The resulting change in voltage generates a pulse. The number of pulses is proportional to the number of cells counted and the size of each pulse is proportional to the volume or size of the cell.7,8
Until recently, analyzers for cell counting have employed optical imaging, scattering, impedance, or a combination of these technologies. In May 2016, FDA granted premarket notification (510(k)) clearance to the GloCyte CSF cell counter by Advanced Instruments, Norwood, Mass, an instrument that offers a new approach to CSF cell counting (see Figure 2). This automated cell counter for CSF uses a combination of fluorescence imaging and a unique sample cartridge. Stained sample is deposited onto a disposable cartridge and vacuum is applied to accelerate the capturing of cells (see Figure 3). The cells captured in the cartridge are then imaged and enumerated by the automated cell counter. (For more information, visit “GloCyte: A Novel Approach.”)
Current Practice and Implications for Patient Care
In current practice, CSF is evaluated macroscopically for color and appearance, followed by microscopic examination for the number of RBCs and WBCs. Based on the macroscopic evaluation, the technologist will decide how to proceed with counting the sample.
CSF is a stat sample; technologists will process the sample immediately by filling both chambers on the hemocytometer—sometimes glass, sometimes plastic—and allowing the cells to settle for 5–10 minutes covered in a petri dish. The two chambers on the hemocytometer allow technologists to perform the count in duplicate (once on each chamber); this practice ensures accuracy and precision, because if one chamber is over- or underfilled, the counts will not match. Both RBCs and WBCs are enumerated on the same hemocytometer (both chambers) and must be within a certain percentage of each other (acceptable percentages vary from one hospital to another). This step alone can delay patient results, because medtechs have to repeat the counts when the sides are different. Another consideration, especially in a busy hospital setting, is that technologists are often under pressure to get results out of the lab; consequently, they might inadvertently bypass the 5–10 minutes required for the cells to settle. This practice can lead to inaccurate results.

Figure 2. The GloCyte System with all the necessary assay components.
Clear and colorless CSF can sometimes be deceiving. In a clear and colorless sample that contains a large number of cells, processing and counting the sample takes more time than expected. Some labs use glacial acetic acid or stain to facilitate counting WBCs. Glacial acetic acid will lyse RBCs and enhance WBCs; while stain will dye WBCs a different color, differentiating them from RBCs. In this case, counting RBCs will be performed on a different hemocytometer. Other labs do not use glacial acetic acid or stain, so counting WBCs is like searching for a needle in a haystack of RBCs. If labs choose to dilute the sample, they may dilute out the WBCs. Not only will that take a long time, but it might also compromise patient results.
If the CSF is bloody, then the technologist has to predict the dilution factor in order to deliver accurate results. Oftentimes, the technologists end up over- or underdiluting the sample. That guessing game can waste valuable time and irretrievable sample. It can take technologists up to an hour to deliver results from a bloody CSF sample—a delay that can compromise patient health.

Figure 3. GloCyte vacuum station captures stained cells on the test cartridge.
Although the manual method is the reference method, it requires trained technologists, is very time consuming and labor-intensive, and it can be very frustrating.
Technologists also have the option to run CSF samples using automated analyzers. In most labs, however, clear and colorless CSF samples are not usually run by automated analyzers due to the limitations of such instruments when handling low cell counts because the instrument is not linear down to zero. Other instruments require a large sample volume or extraneous dilution steps, such as odd dilution factors. Subjectivity is not always excluded from automation, as some current automated analyzers require cell classification, which can result in human error. If the CSF count from current automated analyzers is below what has been validated, or the technologist is not comfortable reporting the results from automation, then they need to go back to the manual method, which requires more sample, more time, and more lab resources.
Future Directions
CSF has been used as a valuable clinical specimen for providing crucial information for diagnosis of a wide variety of infections, diseases, and severe conditions that affect the brain and spinal cord (see Table 2). The information gathered, for any particular clinical diagnosis, and on cell counts, largely depends on the available technologies accepted in the clinical laboratories. Current normal CSF reference ranges were established as accepted clinical guidelines, sometime during the course of using CSF as an aid to diagnosis (see Table 1).
George Hong, PhD, Advanced Instruments.
In this reference range example, however, we may ask how the currently accepted guidelines were established, when no technology has been adequate to provide reliable counts at the considered normal reference range levels. It is known that gold-standard manual microscopy has a coefficient of variation ranging from 20% to 40%, and modern technologies employing flow cytometry are not known to detect accurately down at the reference range for both RBCs and TNCs.9,10
If the normal reference range guidelines were not established using proper technologies, they are certainly subject to challenge until new technologies arrive to confirm them. Fortunately, as new technology continues to arrive on the market, one can search for new ways of providing automated cell counts, beyond flow-cell based ones, for clinical use.
The use of CSF for diagnosis will likely continue because of the beneficial information it provides. Due to the nature of CSF sample requiring a stat result, it will be hugely beneficial for any technology to provide consistent turnaround time, reliable counts down at the low normal reference range for both RBCs and TNCs, and standardization to reduce the person-to-person variability for clinical laboratories.
Julie MacKenzie, MBA, is a product specialist, Reem Kassab, MLS (ASCP), is a hematology application specialist, and George Hong, PhD, is product manager for hematology, at Advanced Instruments, Norwood, Mass. For further information, contact CLP chief editor Steve Halasey via [email protected].
References
- Hajdu SI. A note from history: discovery of the cerebrospinal fluid. Ann Clin Lab Sci. 2003;33(3):334–336. PMID 12956452.
- Brunzel NA. Fundamentals of Urine & Body Fluid Analysis. 3rd ed. St. Louis: Elsevier Saunders, 2013.
- Hussong JW, Kjeldsberg CR. Body Fluids Analysis. Chicago: American Society of Clinical Pathologists, 2015.
- Body Fluid Analysis for Cellular Composition. Approved Guideline H56-A. Wayne, Penn: Clinical and Laboratory Standards Institute, 2006.
- Wallach J. Interpretation of Diagnostic Tests. 6th ed. New York City: Little Brown, 1996.
- Levin MC. Approach to the neurologic patient [online]. In: Merck Manual, Professional Version. (Kenilworth, NJ: Merck Sharp & Dohme, 2016. Available at: www.merckmanuals.com/professional/neurologic-disorders/approach-to-the-neurologic-patient/approach-to-the-neurologic-patient. Accessed January 9, 2017.
- Fleming CKA. From manual microscopy to automated cell counters for first line screening of body fluids: but not without a special body fluid mode. Ned Tijdschr Klin Chem Labgeneesk. 2016;41(3):229–234. Available at: hdl.handle.net/1765/80130.
- Ciesla B. Hematology in Practice. 2nd ed. Philadelphia: FA Davis, 2012.
- Sandhaus LM, Ciarlini P, Kidric D, Dillman C, O’Riordan M. Automated cerebrospinal fluid cell counts using the Sysmex XE-5000: is it time for new reference ranges? Am J Clin Pathol. 2010;134(5):734–738; doi: 10.1309/ajcpabgqxsia4smt.
- Bremell D, Mattsson N, Wallin F, et al. Automated cerebrospinal fluid cell count: new reference ranges and evaluation of its clinical use in central nervous system infections. Clin Biochem. 2014;47(1–2):25–30; doi: 10.1016/j.clinbiochem.2013.11.010.



{kind=link}
Thank you for the regular email updates, it is very useful. continue to keep me updated with latest informations.
THANK YOU.